

Motion correction of in vivo three-dimensional optical coherence tomography of human skin using a fiducial marker
- PMID: 22876343
- PMCID: PMC3409698
- DOI: 10.1364/BOE.3.001774
Motion correction of in vivo three-dimensional optical coherence tomography of human skin using a fiducial marker
Abstract
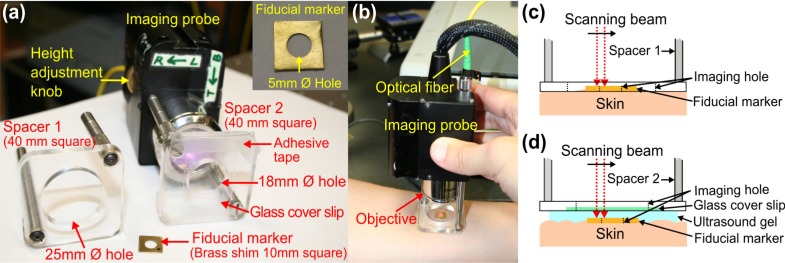
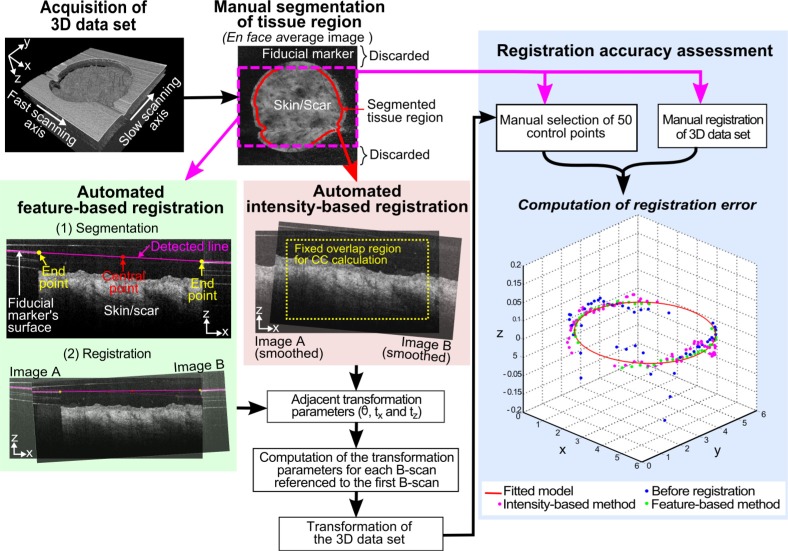
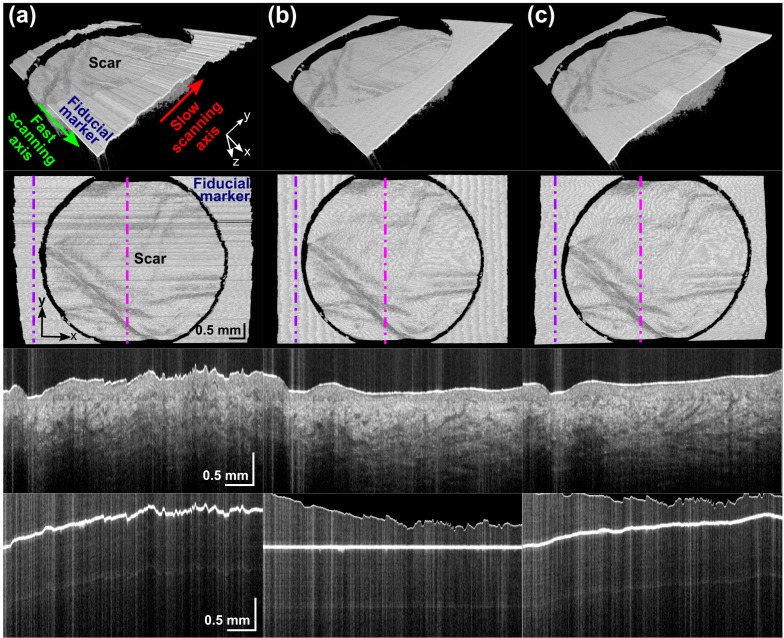
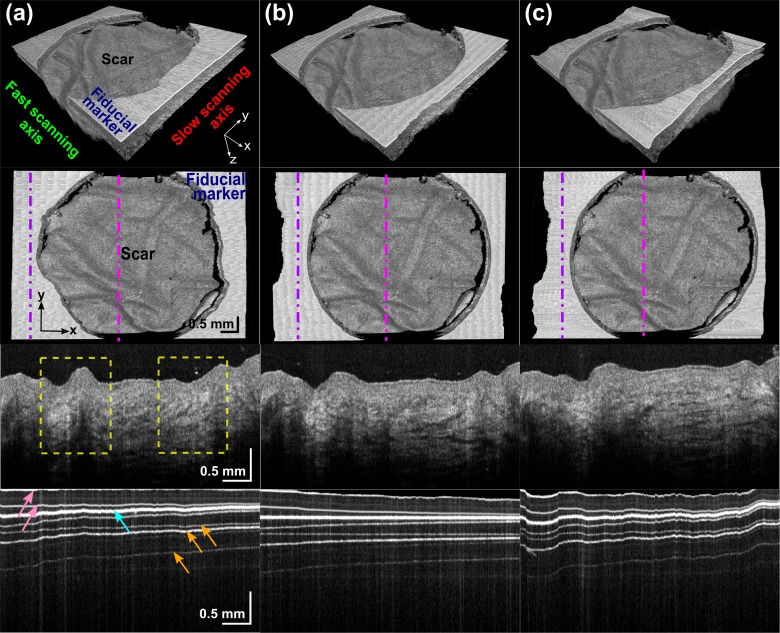
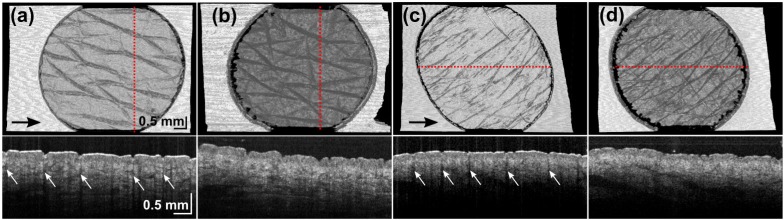
This paper presents a novel method based on a fiducial marker for correction of motion artifacts in 3D, in vivo, optical coherence tomography (OCT) scans of human skin and skin scars. The efficacy of this method was compared against a standard cross-correlation intensity-based registration method. With a fiducial marker adhered to the skin, OCT scans were acquired using two imaging protocols: direct imaging from air into tissue; and imaging through ultrasound gel into tissue, which minimized the refractive index mismatch at the tissue surface. The registration methods were assessed with data from both imaging protocols and showed reduced distortion of skin features due to motion. The fiducial-based method was found to be more accurate and robust, with an average RMS error below 20 µm and success rate above 90%. In contrast, the intensity-based method had an average RMS error ranging from 36 to 45 µm, and a success rate from 50% to 86%. The intensity-based algorithm was found to be particularly confounded by corrugations in the skin. By contrast, tissue features did not affect the fiducial-based method, as the motion correction was based on delineation of the flat fiducial marker. The average computation time for the fiducial-based algorithm was approximately 21 times less than for the intensity-based algorithm.
Keywords: (100.2000) Digital image processing; (100.6950) Tomographic image processing; (170.4500) Optical coherence tomography.
Figures
References
-
- Steiner R., Kunzi-Rapp K., Scharffetter-Kochanek K., “Optical coherence tomography: clinical applications in dermatology,” Med. Laser Appl. 18(3), 249–259 (2003).10.1078/1615-1615-00107 - DOI
-
- Mogensen M., Nürnberg B. M., Forman J. L., Thomsen J. B., Thrane L., Jemec G. B., “In vivo thickness measurement of basal cell carcinoma and actinic keratosis with optical coherence tomography and 20-MHz ultrasound,” Br. J. Dermatol. 160(5), 1026–1033 (2009).10.1111/j.1365-2133.2008.09003.x - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources