

Serological diagnosis of autoimmune bullous skin diseases: prospective comparison of the BIOCHIP mosaic-based indirect immunofluorescence technique with the conventional multi-step single test strategy
- PMID: 22876746
- PMCID: PMC3533694
- DOI: 10.1186/1750-1172-7-49
Serological diagnosis of autoimmune bullous skin diseases: prospective comparison of the BIOCHIP mosaic-based indirect immunofluorescence technique with the conventional multi-step single test strategy
Abstract
Background: Various antigen-specific immunoassays are available for the serological diagnosis of autoimmune bullous diseases. However, a spectrum of different tissue-based and monovalent antigen-specific assays is required to establish the diagnosis. BIOCHIP mosaics consisting of different antigen substrates allow polyvalent immunofluorescence (IF) tests and provide antibody profiles in a single incubation.
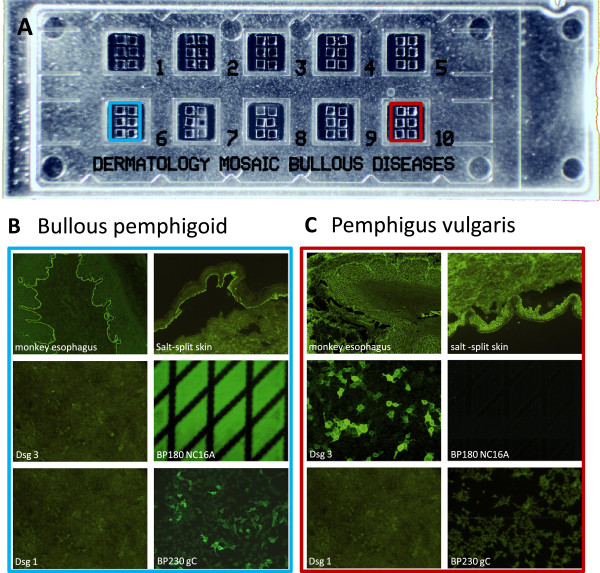
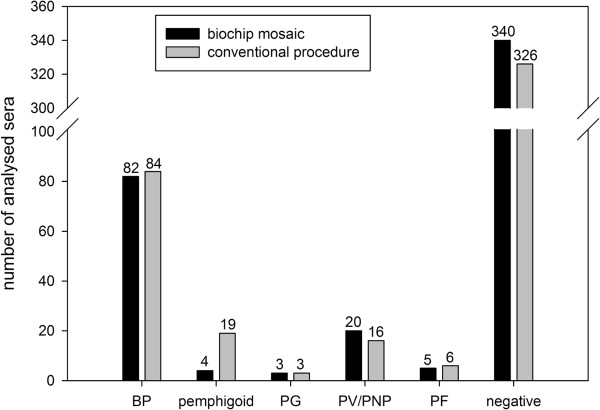
Methods: Slides for indirect IF were prepared, containing BIOCHIPS with the following test substrates in each reaction field: monkey esophagus, primate salt-split skin, antigen dots of tetrameric BP180-NC16A as well as desmoglein 1-, desmoglein 3-, and BP230gC-expressing human HEK293 cells. This BIOCHIP mosaic was probed using a large panel of sera from patients with pemphigus vulgaris (PV, n=65), pemphigus foliaceus (PF, n=50), bullous pemphigoid (BP, n=42), and non-inflammatory skin diseases (n=97) as well as from healthy blood donors (n=100). Furthermore, to evaluate the usability in routine diagnostics, 454 consecutive sera from patients with suspected immunobullous disorders were prospectively analyzed in parallel using a) the IF BIOCHIP mosaic and b) a panel of single antibody assays as commonly used by specialized centers.
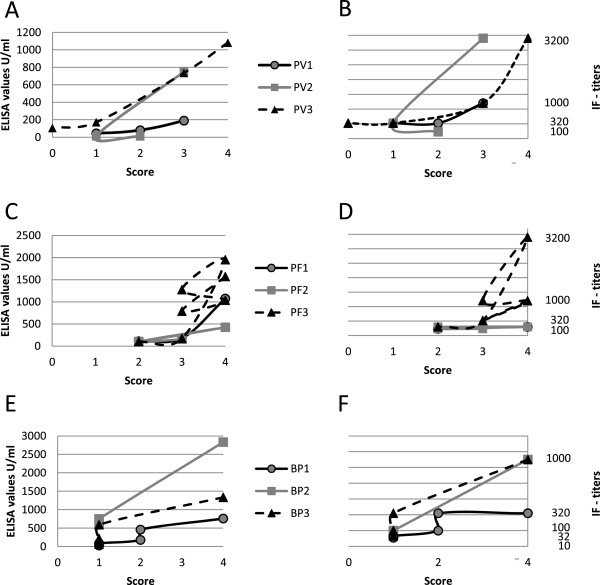
Results: Using the BIOCHIP mosaic, sensitivities of the desmoglein 1-, desmoglein 3-, and NC16A-specific substrates were 90%, 98.5% and 100%, respectively. BP230 was recognized by 54% of the BP sera. Specificities ranged from 98.2% to 100% for all substrates. In the prospective study, a high agreement was found between the results obtained by the BIOCHIP mosaic and the single test panel for the diagnosis of BP, PV, PF, and sera without serum autoantibodies (Cohen's κ between 0.88 and 0.97).
Conclusions: The BIOCHIP mosaic contains sensitive and specific substrates for the indirect IF diagnosis of BP, PF, and PV. Its diagnostic accuracy is comparable with the conventional multi-step approach. The highly standardized and practical BIOCHIP mosaic will facilitate the serological diagnosis of autoimmune blistering diseases.
Figures
References
-
- Eming R, Hertl M. Autoimmune bullous disorders. Clin Chem Lab Med. 2006;44:144–149. - PubMed
-
- Kanwar AJ, De D. Pemphigus in India. Indian J Dermatol Venereol Leprol. 2011;77:439–449. - PubMed
-
- Marazza G, Pham HC, Scharer L, Pedrazzetti PP, Hunziker T, Trueb RM, Hohl D, Itin P, Lautenschlager S, Naldi L, Borradori L. Incidence of bullous pemphigoid and pemphigus in Switzerland: a 2-year prospective study. Br J Dermatol. 2009;161:861–868. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
