

Review
doi: 10.1016/j.ecl.2012.05.001.
Epub 2012 Jun 17.
Male osteoporosis
Affiliations
- PMID: 22877433
- PMCID: PMC3602974
- DOI: 10.1016/j.ecl.2012.05.001
Item in Clipboard
Review
Male osteoporosis
Endocrinol Metab Clin North Am.
2012 Sep.
Abstract
Osteoporosis is now recognized as a major threat to health in aging men. Morbidity and mortality, particularly following hip fracture, are substantial. Although trabecular bone loss starts in early adulthood, loss of cortical bone only seems to occur from midlife onwards. Declining bioavailable estradiol levels plays an integral role in male age-associated bone loss. Both pharmacologic and supportive care interventions are important for optimal care in men at an increased fracture risk.
Copyright © 2012 Elsevier Inc. All rights reserved.
Figures
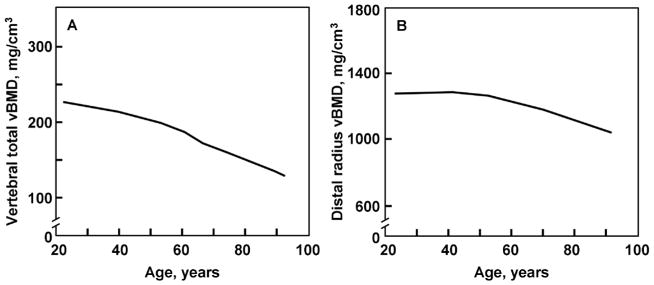
A. Total vertebral body vBMD values (mg/cm3) from a population sample (n=323) of Rochester, Minnesota men aged 20–97 years. B. Cortical vBMD values at the distal radius in the same male cohort. Adapted from Riggs et al. (2004) J Bone Miner Res. 19:1945–1954 with permission from the American Society of Bone and Mineral Research.
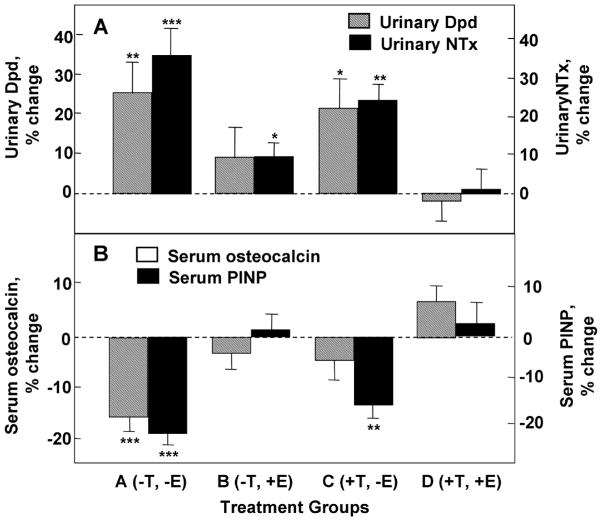
Percent changes in markers of (A) bone resorption (urinary deoxypyridinoline [Dpd] and N-telopeptide of type I collagen [NTX] and (B) bone formation (serum osteocalcin and N-terminal extension peptide of type I collagen [P1NP]) in elderly men (mean age, 68 years) pharmacologically made acutely hypogonadal and subsequently treated with either an aromatase inhibitor (group A), estrogen alone (group B), testosterone alone (group C), or both estrogen and testosterone (group D). Significance for change from baseline: *, p < 0.05; **, p < 0.01; ***, p < 0.001. Adapted from Falahati-Nini et al. (2000) J Clin Invest 106:1553–1560 with permission from the American Society for Clinical Investigation.
References
-
- Consensus development conference: diagnosis, prophylaxis, and treatment of osteoporosis. Am J Med. 1993;94(6):646–650. - PubMed
-
- Melton LJ, 3rd, Khosla S, Achenbach SJ, et al. Effects of body size and skeletal site on the estimated prevalence of osteoporosis in women and men. Osteoporos Int. 2000;11(11):977–983. - PubMed
-
- Cooper C, Campion G, Melton LJ., 3rd Hip fractures in the elderly: a world-wide projection. Osteoporos Int. 1992;2(6):285–289. - PubMed
-
- Johnell O, Kanis JA. An estimate of the worldwide prevalence, mortality and disability associated with hip fracture. Osteoporos Int. 2004;15(11):897–902. - PubMed
-
- Johnell O, Kanis JA. An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos Int. 2006;17(12):1726–1733. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
