

Cortical microstructure and estimated bone strength in young amenorrheic athletes, eumenorrheic athletes and non-athletes
- PMID: 22878154
- PMCID: PMC3482939
- DOI: 10.1016/j.bone.2012.07.019
Cortical microstructure and estimated bone strength in young amenorrheic athletes, eumenorrheic athletes and non-athletes
Abstract
Context: Lower bone density in young amenorrheic athletes (AA) compared to eumenorrheic athletes (EA) and non-athletes may increase fracture risk during a critical time of bone accrual. Finite element analysis (FEA) is a unique tool to estimate bone strength in vivo, and the contribution of cortical microstructure to bone strength in young athletes is not well understood.
Objective: We hypothesized that FEA-estimated stiffness and failure load are impaired in AA at the distal radius and tibia compared to EA and non-athletes despite weight-bearing exercise.
Design and setting: Cross-sectional study; Clinical Research Center
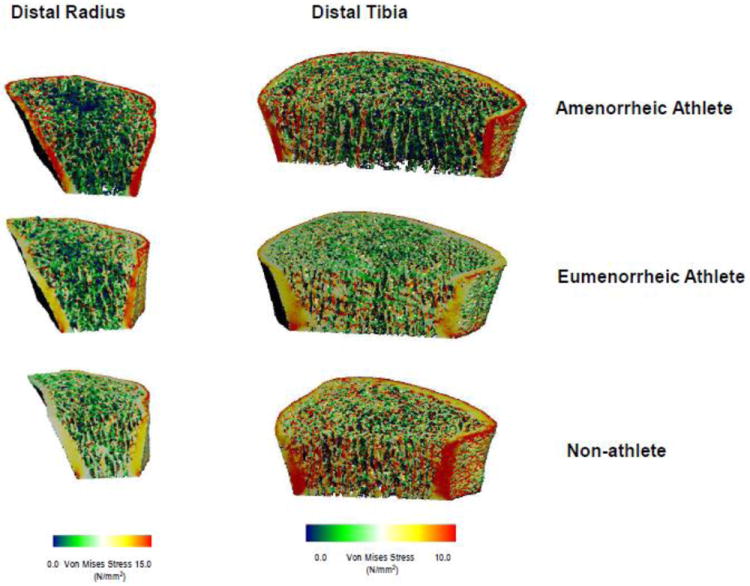
Subjects: 34 female endurance athletes involved in weight-bearing sports (17 AA, 17 EA) and 16 non-athletes (14-21 years) of comparable age, maturity and BMI OUTCOME MEASURES: We used HR-pQCT images to assess cortical microarchitecture and FEA to estimate bone stiffness and failure load.
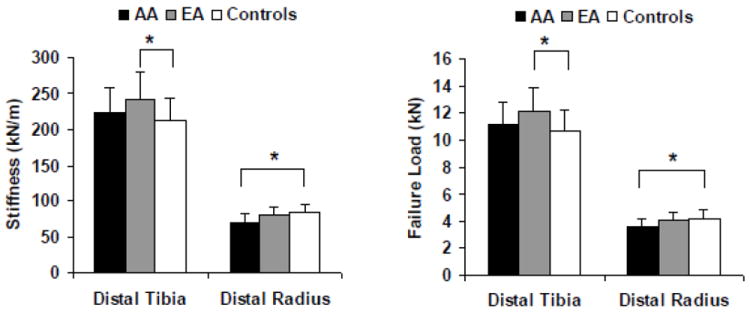
Results: Cortical perimeter, porosity and trabecular area at the weight-bearing tibia were greater in both groups of athletes than non-athletes, whereas the ratio (%) of cortical to total area was lowest in AA. Despite greater cortical porosity in EA, estimated tibial stiffness and failure load was higher than in non-athletes. However, this advantage was lost in AA. At the non-weight-bearing radius, failure load and stiffness were lower in AA than non-athletes. After controlling for lean mass and menarchal age, athletic status accounted for 5-9% of the variability in stiffness and failure load, menarchal age for 8-23%, and lean mass for 12-37%.
Conclusion: AA have lower FEA-estimated bone strength at the distal radius than non-athletes, and lose the advantage of weight-bearing exercise seen in EA at the distal tibia.
Copyright © 2012 Elsevier Inc. All rights reserved.
Conflict of interest statement
All authors state that they have no conflicts of interest.
Figures
References
-
- Harel Z, Gold M, Cromer B, Bruner A, Stager M, Bachrach L, Wolter K, Reid C, Hertweck P, Nelson A, Nelson D, Coupey S, Johnson C, Burkman R, Bone H. Bone mineral density in postmenarchal adolescent girls in the United States: associated biopsychosocial variables and bone turnover markers. J Adolesc Health. 2007;40:44–53. - PubMed
-
- Whiting SJ, Vatanparast H, Baxter-Jones A, Faulkner RA, Mirwald R, Bailey DA. Factors that affect bone mineral accrual in the adolescent growth spurt. J Nutr. 2004;134:696S–700S. - PubMed
-
- Nichols DL, Bonnick SL, Sanborn CF. Bone health and osteoporosis. Clin Sports Med. 2000;19:233–49. - PubMed
-
- Nichols DL, Sanborn CF, Essery EV. Bone density and young athletic women. An update. Sports Med. 2007;37:1001–14. - PubMed
-
- Johnston CC, Jr, Slemenda CW. Peak bone mass, bone loss and risk of fracture. Osteoporos Int. 1994;4(Suppl 1):43–5. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
