

The relationship between components of tumour inflammatory cell infiltrate and clinicopathological factors and survival in patients with primary operable invasive ductal breast cancer
- PMID: 22878371
- PMCID: PMC3426752
- DOI: 10.1038/bjc.2012.347
The relationship between components of tumour inflammatory cell infiltrate and clinicopathological factors and survival in patients with primary operable invasive ductal breast cancer
Abstract
Background: The importance of the components of host local inflammatory response in determining outcome in primary operable ductal invasive breast cancer is not clear. The aim of this study was to examine the relationship between components of the tumour inflammatory cell infiltrate and standard clinicopathological factors including hormone status (oestrogen receptor (ER), progesterone receptor (PR) and human epidermal growth factor receptor (HER)-2), Ki-67 and survival in patients with primary operable invasive ductal breast cancer.
Methods: Tumour inflammatory cell infiltrate, hormone status (ER, PR and HER-2), Ki-67 and standard clinicopathological factors were determined using routine pathological and immuno-histochemical techniques in 468 patients.
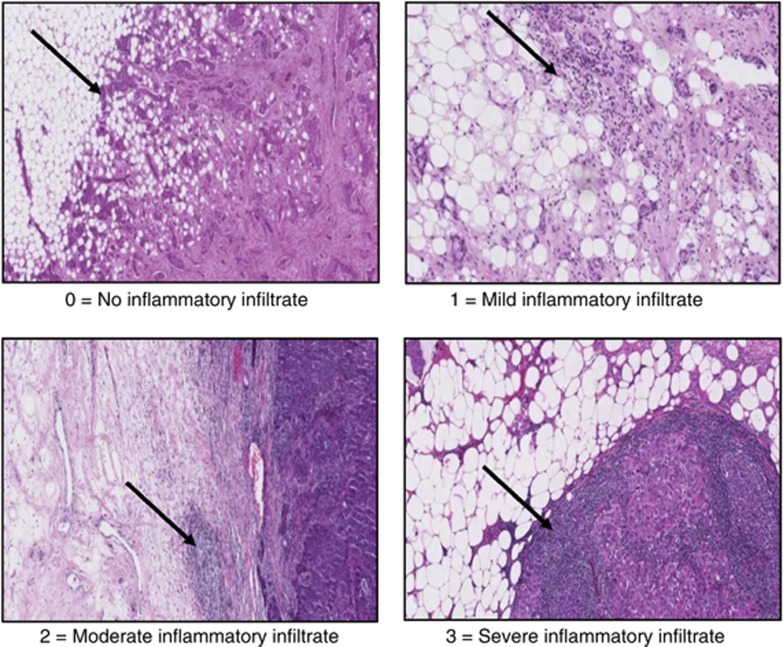
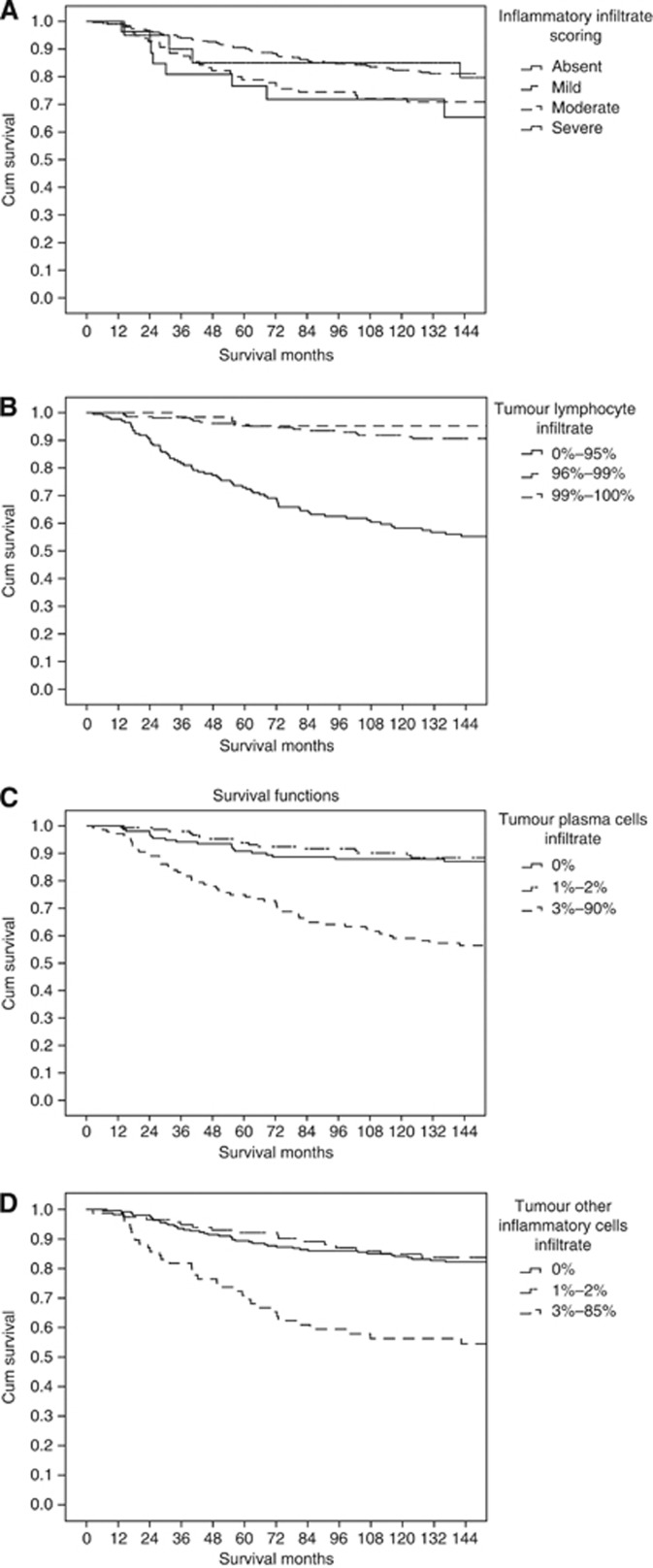
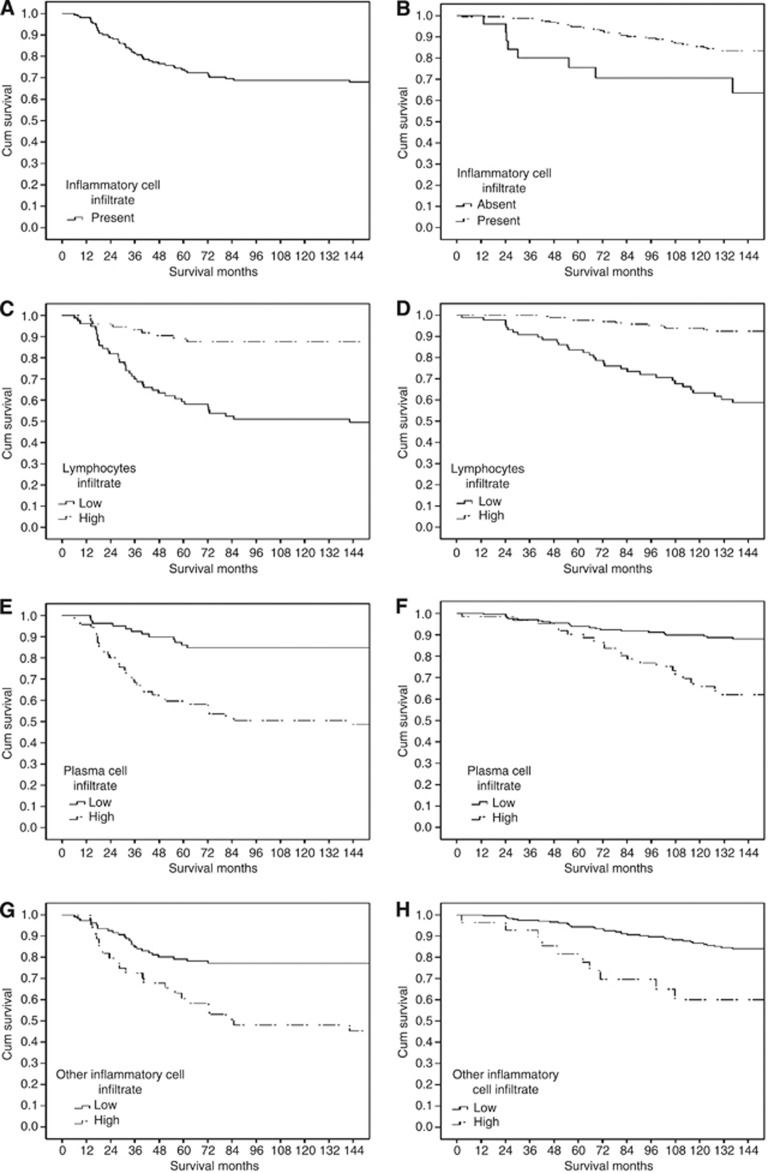
Results: The large majority (94%) of ductal tumours had evidence of inflammatory cell infiltrate. The general inflammatory cell infiltrate was positively associated with high grade (P<0.001), the absence of ER (P<0.001), the absence of PR (P<0.01), the presence of vascular invasion (P<0.05) and high lymphocytic infiltrate, plasma cell infiltrate, other inflammatory cell infiltrate and macrophage infiltrate (all P<0.001). The median follow-up of the survivors was 165 months. During this period, 93 patients died of their cancer. On univariate analysis, stratified for ER status, tumour size (P<0.01), lymph node involvement (P<0.001), tumour plasma cell infiltrate (P<0.001), other inflammatory cell infiltrate (P<0.05) and treatment (P<0.05) were associated with poorer cancer-specific survival whereas lymphocyte infiltrate (P<0.001) was associated with improved cancer-specific survival. On multivariate analysis, stratified for ER status, lymph node involvement (P<0.05) was independently associated with poorer cancer-specific survival whereas increased tumour lymphocyte infiltrate (P<0.001) was independently associated with improved cancer-specific survival.
Conclusion: The results of this study show that, using routine histology, the general inflammatory cell infiltrate was a common feature and was positively associated with high grade, the absence of ER, the absence of PR, the presence of vascular invasion and high-grade infiltration of lymphocytes, plasma cells, other inflammatory cells and macrophages. Also, that within a mature cohort of patients, a high lymphocytic infiltrate was associated with improved survival, independent of clinicopathological characteristics including ER status, in primary operable ductal invasive breast cancer. These results rationalise previous work and provide a sound basis for future studies in this important area of breast cancer research.
Figures
References
-
- Cancerstats (2008) http://info.cancerresearchuk.org/cancerstats/types/breast/incidence. Accessed 25 June 2010
-
- Colotta F, Allavena P, Sica A, Garlanda C, Mantovani A (2009) Cancer-related inflammation, the seventh hallmark of cancer: links to genetic instability. Carcinogenesis 30(7): 1073–1081 - PubMed
-
- de Visser KE, Korets LV, Coussens LM (2005) De novo carcinogenesis promoted by chronic inflammation is B lymphocyte dependent. Cancer Cell 7(5): 411–423 - PubMed
-
- Dong HP, Elstrand MB, Holth A, Silins I, Berner A, Trope CG, Davidson B, Risberg Br (2006) NK- and B-cell infiltration correlates with worse outcome in metastatic ovarian carcinoma. Am J Clin Pathol 125(3): 451–458 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
