

T cell profiling reveals high CD4+CTLA-4 + T cell frequency as dominant predictor for survival after prostate GVAX/ipilimumab treatment
- PMID: 22878899
- PMCID: PMC11029684
- DOI: 10.1007/s00262-012-1330-5
T cell profiling reveals high CD4+CTLA-4 + T cell frequency as dominant predictor for survival after prostate GVAX/ipilimumab treatment
Abstract
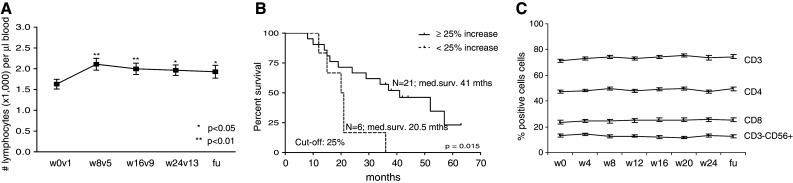
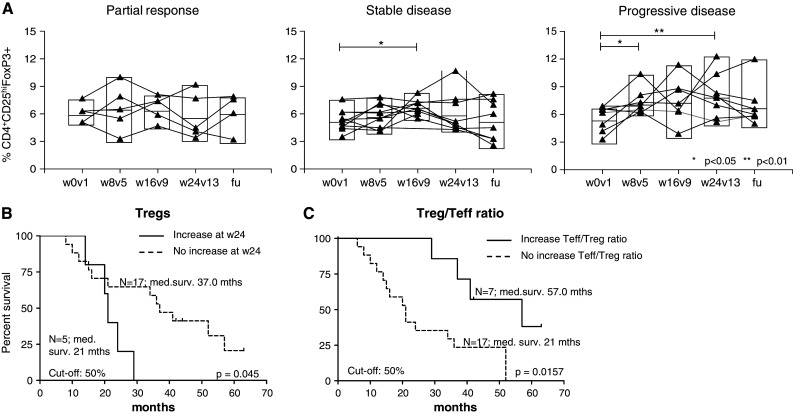
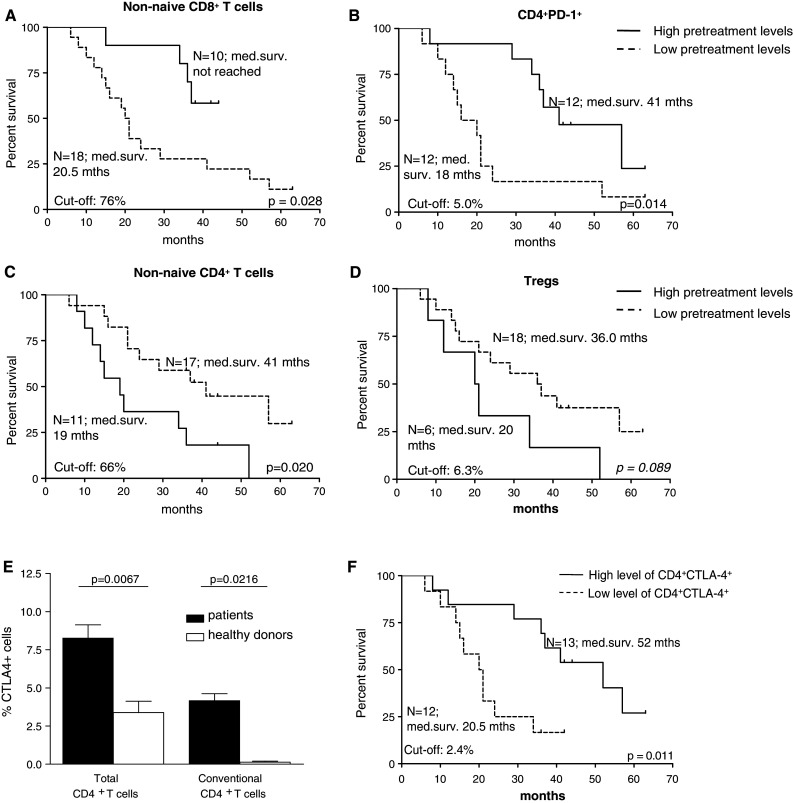
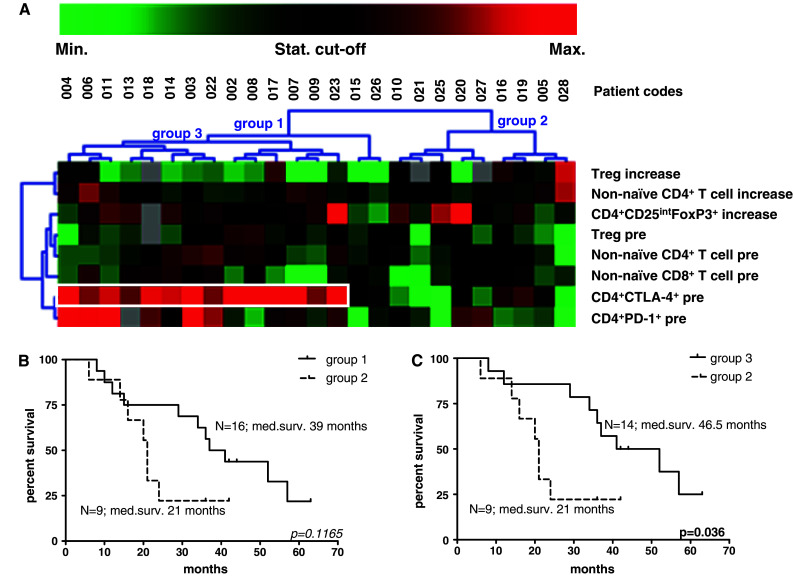
Immune checkpoint blockade enhances antitumor responses, but can also lead to severe immune-related adverse events (IRAE). To avoid unnecessary exposure to these potentially hazardous agents, it is important to identify biomarkers that correlate with clinical activity and can be used to select patients that will benefit from immune checkpoint blockade. To understand the consequences of CTLA-4 blockade and identify biomarkers for clinical efficacy and/or survival, an exploratory T cell monitoring study was performed in a phase I/II dose escalation/expansion trial (n = 28) of combined Prostate GVAX/ipilimumab immunotherapy. Phenotypic T cell monitoring in peripheral blood before and after Prostate GVAX/ipilimumab treatment revealed striking differences between patients who benefited from therapy and patients that did not. Treatment-induced rises in absolute lymphocyte counts, CD4(+) T cell differentiation, and CD4(+) and CD8(+) T cell activation were all associated with clinical benefit. Moreover, significantly prolonged overall survival (OS) was observed for patients with high pre-treatment frequencies of CD4(+)CTLA-4(+), CD4(+)PD-1(+), or differentiated (i.e., non-naive) CD8(+) T cells or low pre-treatment frequencies of differentiated CD4(+) or regulatory T cells. Unsupervised clustering of these immune biomarkers revealed cancer-related expression of CTLA-4(+) in CD4(+) T cells to be a dominant predictor for survival after Prostate GVAX/ipilimumab therapy and to thus provide a putative and much-needed biomarker for patient selection prior to therapeutic CTLA4 blockade.
Conflict of interest statement
J. M. C. is a Bristol-Myers Squibb employee, and J. M. C and I. L. own stock and/or stock options from Bristol-Myers Squibb. A.J.M.v.d.E. and W.R.G. have served as consultants and received honoraria from Bristol-Myers Squibb. T.D.G and W.R.G. received an educational grant from Cell Genesys Inc. All other authors declare that they have no conflict of interest.
Figures
References
-
- Kantoff PW, Schuetz TJ, Blumenstein BA, Glode LM, Bilhartz DL, Wyand M, Manson K, Panicali DL, Laus R, Schlom J, Dahut WL, Arlen PM, Gulley JL, Godfrey WR. Overall survival analysis of a phase II randomized controlled trial of a Poxviral-based PSA-targeted immunotherapy in metastatic castration-resistant prostate cancer. J Clin Oncol. 2010;28:1099–1105. doi: 10.1200/JCO.2009.25.0597. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
