

Targeting mannose-binding lectin confers long-lasting protection with a surprisingly wide therapeutic window in cerebral ischemia
- PMID: 22879370
- PMCID: PMC3478764
- DOI: 10.1161/CIRCULATIONAHA.112.103051
Targeting mannose-binding lectin confers long-lasting protection with a surprisingly wide therapeutic window in cerebral ischemia
Abstract
Background: The involvement of the complement system in brain injury has been scarcely investigated. Here, we document the pivotal role of mannose-binding lectin (MBL), one of the recognition molecules of the lectin complement pathway, in brain ischemic injury.
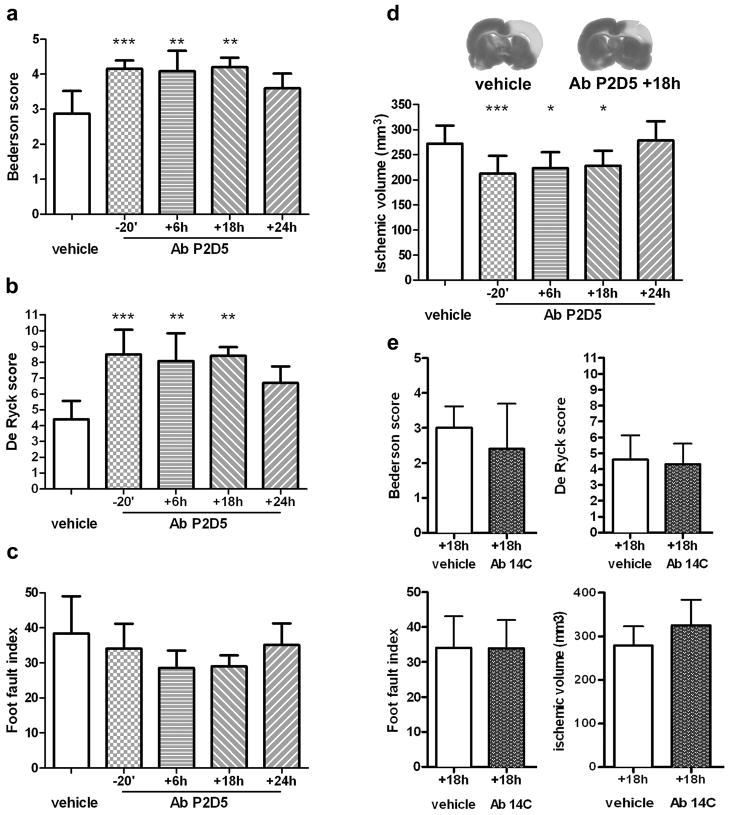
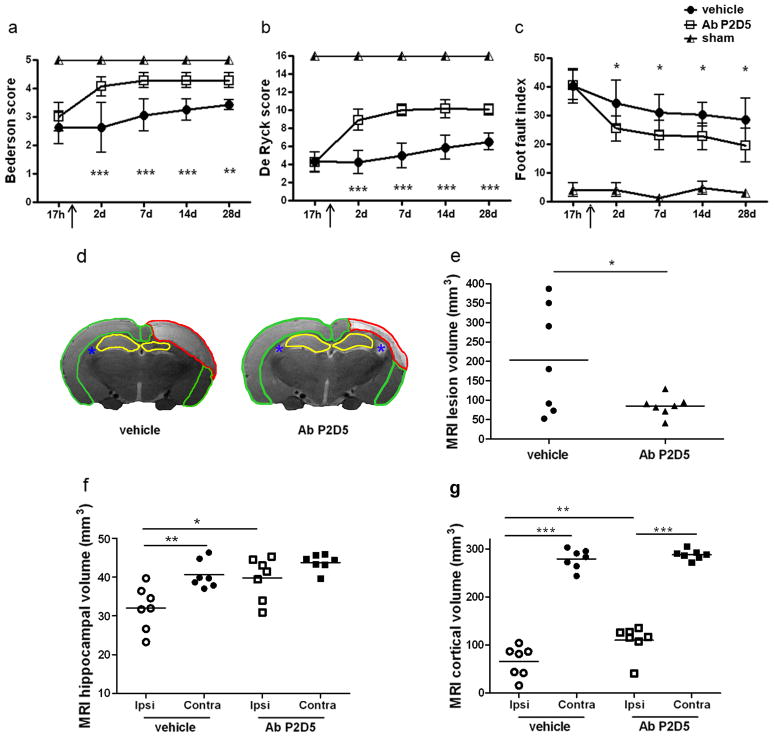
Methods and results: Focal cerebral ischemia was induced in mice (by permanent or transient middle cerebral artery occlusion) and rats (by 3-vessel occlusion). We first observed that MBL is deposited on ischemic vessels up to 48 hours after injury and that functional MBL/MBL-associated serine protease 2 complexes are increased. Next, we demonstrated that (1) MBL(-/-) mice are protected from both transient and permanent ischemic injury; (2) Polyman2, the newly synthesized mannosylated molecule selected for its binding to MBL, improves neurological deficits and infarct volume when given up to 24 hours after ischemia in mice; (3) anti-MBL-A antibody improves neurological deficits and infarct volume when given up to 18 hours after ischemia, as assessed after 28 days in rats.
Conclusions: Our data show an important role for MBL in the pathogenesis of brain ischemic injury and provide a strong support to the concept that MBL inhibition may be a relevant therapeutic target in humans, one with a wide therapeutic window of application.
Conflict of interest statement
Figures




References
-
- Lo EH. A new penumbra: transitioning from injury into repair after stroke. Nat Med. 2008;14:497–500. - PubMed
-
- Lees JS, Mishra NK, Saini M, Lyden PD, Shuaib A. Low body temperature does not compromise the treatment effect of alteplase. Stroke. 2011;42:2618–2621. - PubMed
-
- Fonarow GC, Smith EE, Saver JL, Reeves MJ, Bhatt DL, Grau-Sepulveda MV, Olson DM, Hernandez AF, Peterson ED, Schwamm LH. Timeliness of tissue-type plasminogen activator therapy in acute ischemic stroke: patient characteristics, hospital factors, and outcomes associated with door-to-needle times within 60 minutes. Circulation. 2011;123:750–758. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Miscellaneous
