

Four-dimensional blood flow-specific markers of LV dysfunction in dilated cardiomyopathy
- PMID: 22879457
- PMCID: PMC3626338
- DOI: 10.1093/ehjci/jes159
Four-dimensional blood flow-specific markers of LV dysfunction in dilated cardiomyopathy
Abstract
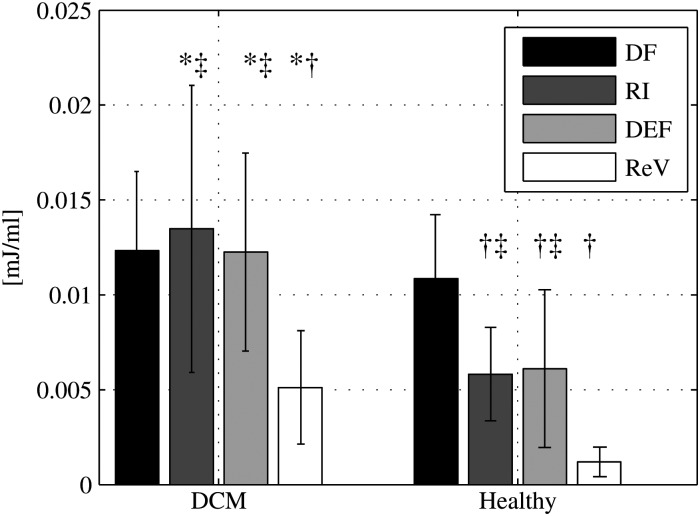
Aims: Patients with mild heart failure (HF) who are clinically compensated may have normal left ventricular (LV) stroke volume (SV). Despite this, altered intra-ventricular flow patterns have been recognized in these subjects. We hypothesized that, compared with normal LVs, flow in myopathic LVs would demonstrate a smaller proportion of inflow volume passing directly to ejection and diminished the end-diastolic preservation of the inflow kinetic energy (KE).
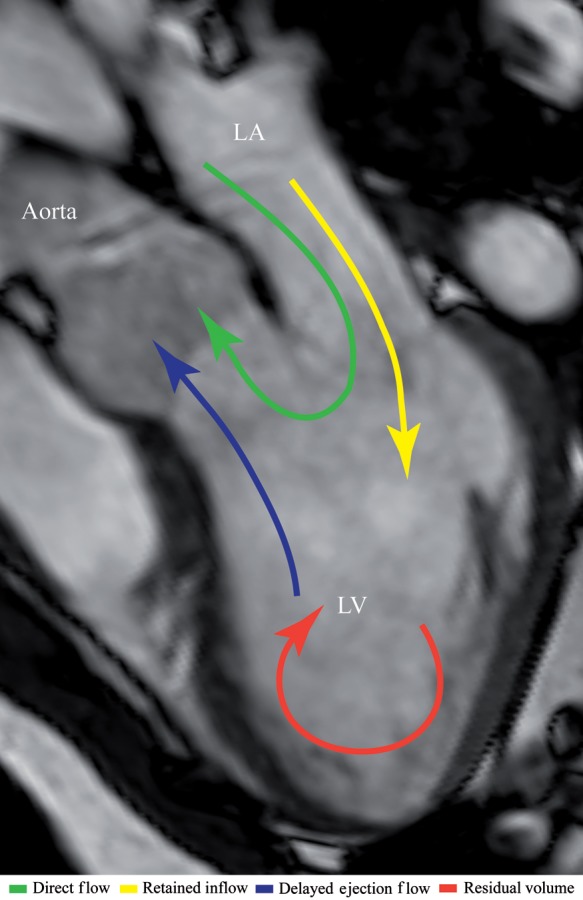
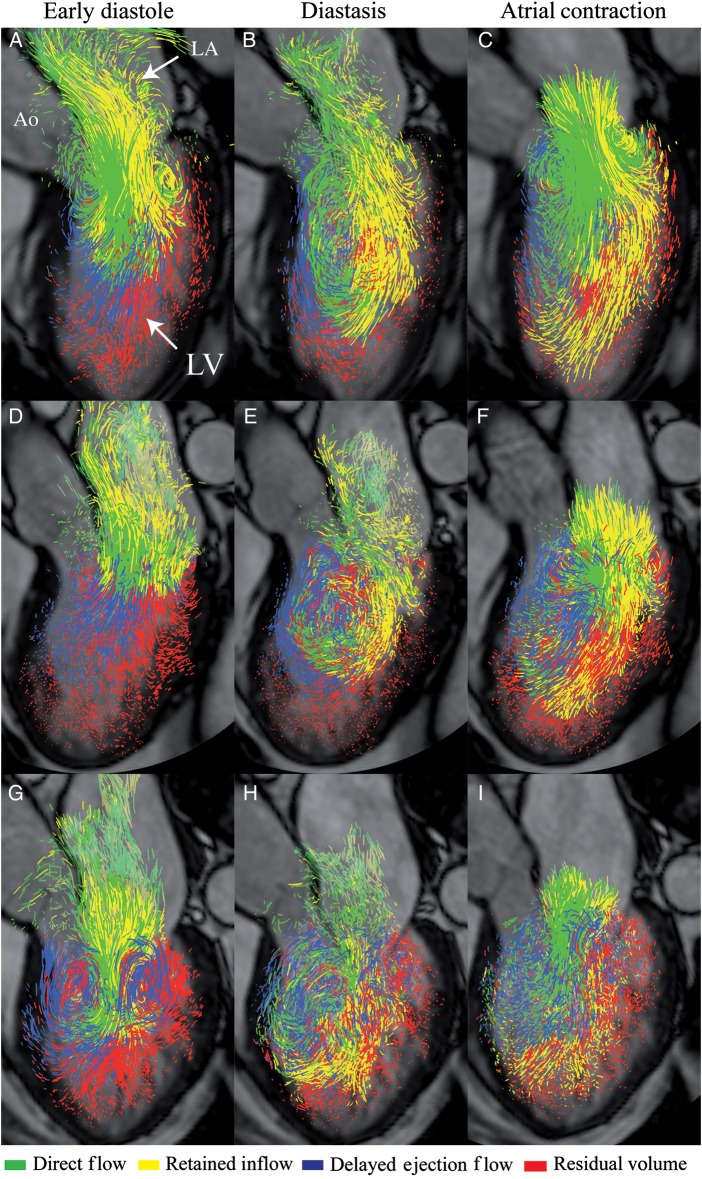
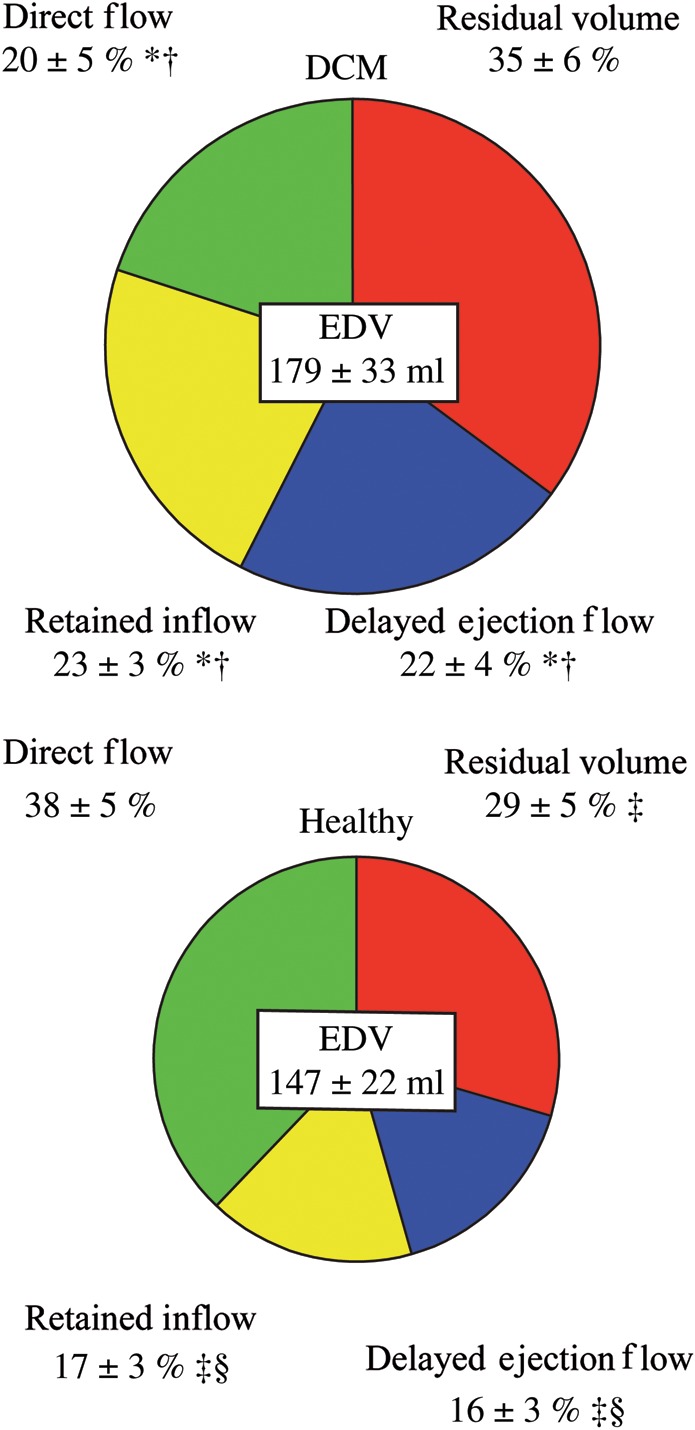
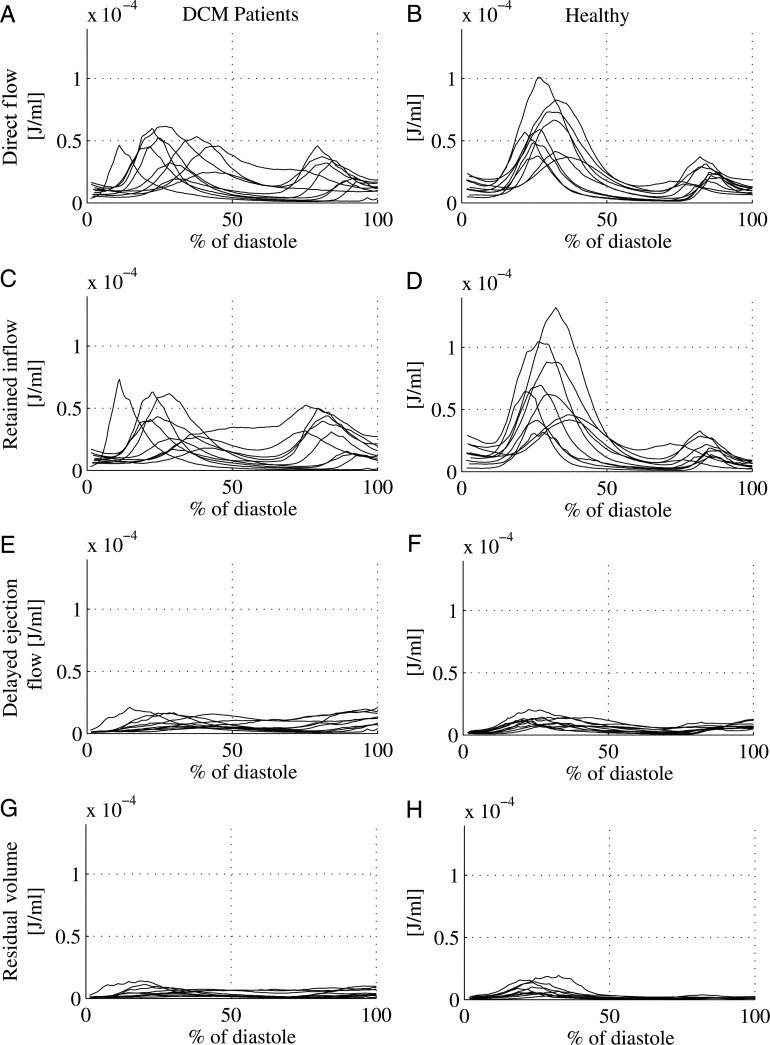
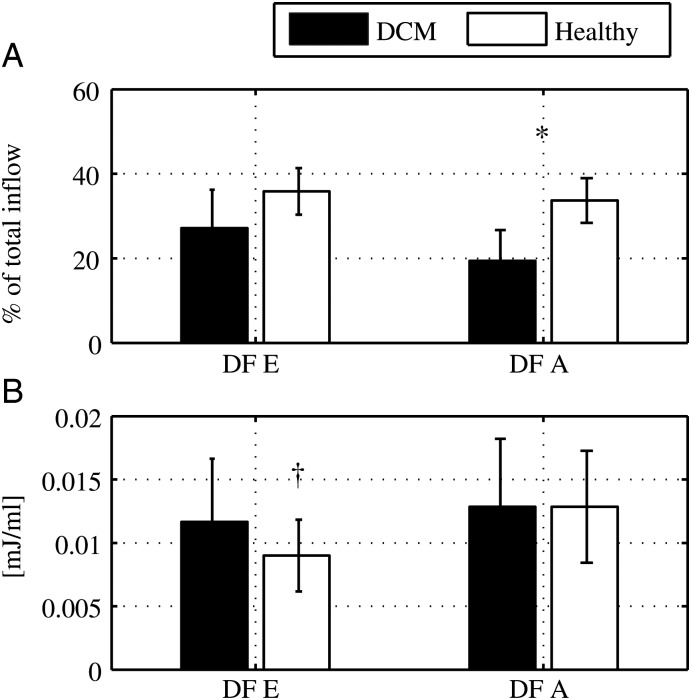
Methods and results: In 10 patients with dilated cardiomyopathy (DCM) (49 ± 14 years, six females) and 10 healthy subjects (44 ± 17 years, four females), four-dimensional MRI velocity and morphological data were acquired. A previously validated method was used to separate the LV end-diastolic volume (EDV) into four flow components based on the blood's locations at the beginning and end of the cardiac cycle. KE was calculated over the cardiac cycle for each component. The EDV was larger (P = 0.021) and the ejection fraction smaller (P < 0.001) in DCM compared with healthy subjects; the SV was equivalent (DCM: 77 ± 19, healthy: 79 ± 16 mL). The proportion of the total LV inflow that passed directly to ejection was smaller in DCM (P = 0.000), but the end-diastolic KE/mL of the direct flow was not different in the two groups (NS).
Conclusion: Despite equivalent LVSVs, HF patients with mild LV remodelling demonstrate altered diastolic flow routes through the LV and impaired preservation of inflow KE at pre-systole compared with healthy subjects. These unique flow-specific changes in the flow route and energetics are detectable despite clinical compensation, and may prove useful as subclinical markers of LV dysfunction.
Figures
References
-
- Stewart S, MacIntyre K, Hole DJ, Capewell S, McMurray JJ. More ‘malignant’ than cancer? Five-year survival following a first admission for heart failure. Eur J Heart Fail. 2001;3:315–22. doi:10.1016/S1388-9842(00)00141-0. - DOI - PubMed
-
- Hill JA, Olson EN. Cardiac plasticity. N Engl J Med. 2008;58:1370–80. doi:10.1056/NEJMra072139. - DOI - PubMed
-
- Richter Y, Edelman ER. Cardiology is flow. Circulation. 2006;113:2679–82. doi:10.1161/CIRCULATIONAHA.106.632687. - DOI - PubMed
-
- Kilner PJ, Yang GZ, Wilkes AJ, Mohiaddin RH, Firmin DN, Yacoub MH. Asymmetric redirection of flow through the heart. Nature. 2000;404:759–61. doi:10.1038/35008075. - DOI - PubMed
-
- Mohiaddin RH. Flow patterns in the dilated ischemic left ventricle studied by MR imaging with velocity vector mapping. J Magn Reson Imaging. 1995;5:493–8. doi:10.1002/jmri.1880050503. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
