

Feasibility, yield, and cost of active tuberculosis case finding linked to a mobile HIV service in Cape Town, South Africa: a cross-sectional study
- PMID: 22879816
- PMCID: PMC3413719
- DOI: 10.1371/journal.pmed.1001281
Feasibility, yield, and cost of active tuberculosis case finding linked to a mobile HIV service in Cape Town, South Africa: a cross-sectional study
Abstract
Background: The World Health Organization is currently developing guidelines on screening for tuberculosis disease to inform national screening strategies. This process is complicated by significant gaps in knowledge regarding mass screening. This study aimed to assess feasibility, uptake, yield, treatment outcomes, and costs of adding an active tuberculosis case-finding program to an existing mobile HIV testing service.
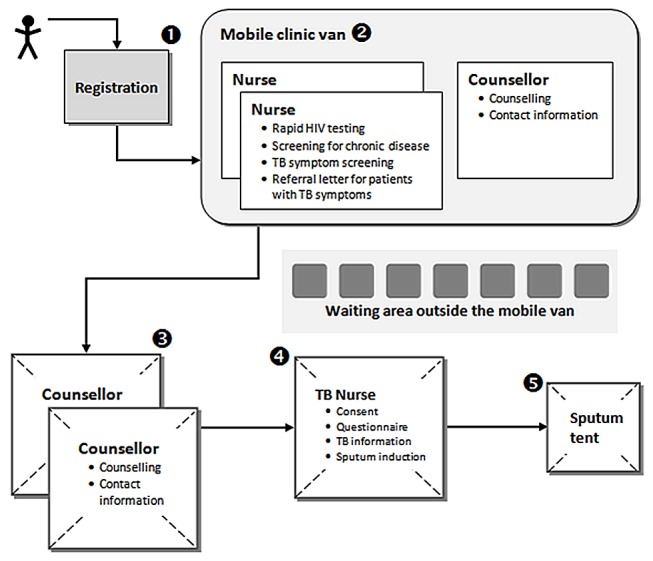
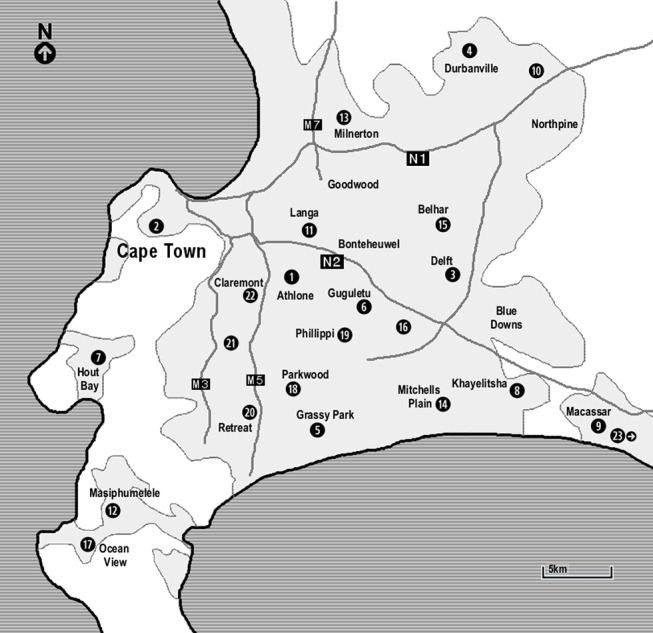
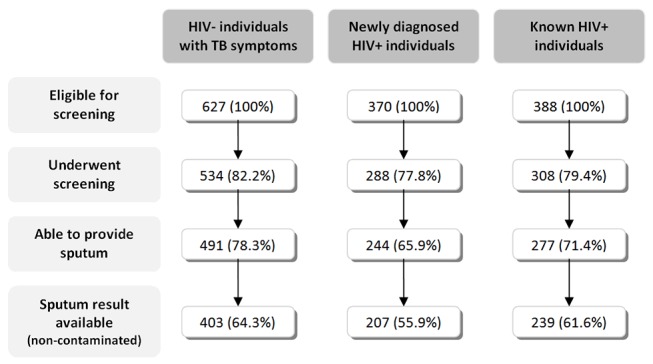
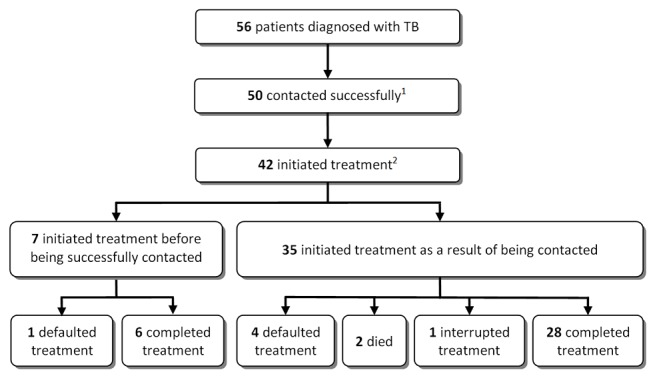
Methods and findings: The study was conducted at a mobile HIV testing service operating in deprived communities in Cape Town, South Africa. All HIV-negative individuals with symptoms suggestive of tuberculosis, and all HIV-positive individuals regardless of symptoms were eligible for participation and referred for sputum induction. Samples were examined by microscopy and culture. Active tuberculosis case finding was conducted on 181 days at 58 different sites. Of the 6,309 adults who accessed the mobile clinic, 1,385 were eligible and 1,130 (81.6%) were enrolled. The prevalence of smear-positive tuberculosis was 2.2% (95% CI 1.1-4.0), 3.3% (95% CI 1.4-6.4), and 0.4% (95% CI 1.4 015-6.4) in HIV-negative individuals, individuals newly diagnosed with HIV, and known HIV, respectively. The corresponding prevalence of culture-positive tuberculosis was 5.3% (95% CI 3.5-7.7), 7.4% (95% CI 4.5-11.5), 4.3% (95% CI 2.3-7.4), respectively. Of the 56 new tuberculosis cases detected, 42 started tuberculosis treatment and 34 (81.0%) completed treatment. The cost of the intervention was US$1,117 per tuberculosis case detected and US$2,458 per tuberculosis case cured. The generalisability of the study is limited to similar settings with comparable levels of deprivation and TB and HIV prevalence.
Conclusions: Mobile active tuberculosis case finding in deprived populations with a high burden of HIV and tuberculosis is feasible, has a high uptake, yield, and treatment success. Further work is now required to examine cost-effectiveness and affordability and whether and how the same results may be achieved at scale.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- WHO Three I's Meeting (2008) Geneva: World Health Organization. Available: http://www.who.int/hiv/pub/meetingreports/WHO_3Is_meeting_report.pdf. Accessed 31 August 2011.
-
- WHO (2010) Guidelines for intensified tuberculosis case-finding and isoniazid preventive therapy for people living with HIV in resource-constrained settings. Geneva: World Health Organization. Available: http://www.who.int/hiv/pub/tb/9789241500708/en/index.html. Accessed 20 February 2011.
-
- International Union Against Tuberculosis and Lung Disease (2007) Best practice for the care of patients with tuberculosis: a guide for low-income countries. Paris: International Union Against Tuberculosis and Lung Disease. Available: http://www.theunion.org/index.php/en/resources/scientific-publications/t.... Accessed 21/9/2011.
-
- International Union Against Tuberculosis and Lung Disease (2002) Interventions for TB control and elimination. Paris: International Union Against Tuberculosis and Lung Disease. Available: http://www.tbrieder.org/publications/books_english/interventions.pdf. Accessed 21/9/2011.
-
- WHO (2006) Guidance for national tuberculosis programmes on the management of tuberculosis in children. Geneva: World Health Organization. Available: http://whqlibdoc.who.int/hq/2006/WHO_HTM_TB_2006.371_eng.pdf. Accessed 21/9/2011. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
