

In the face of chronic aspiration, prolonged ischemic time exacerbates obliterative bronchiolitis in rat pulmonary allografts
- PMID: 22882880
- PMCID: PMC4332511
- DOI: 10.1111/j.1600-6143.2012.04215.x
In the face of chronic aspiration, prolonged ischemic time exacerbates obliterative bronchiolitis in rat pulmonary allografts
Abstract
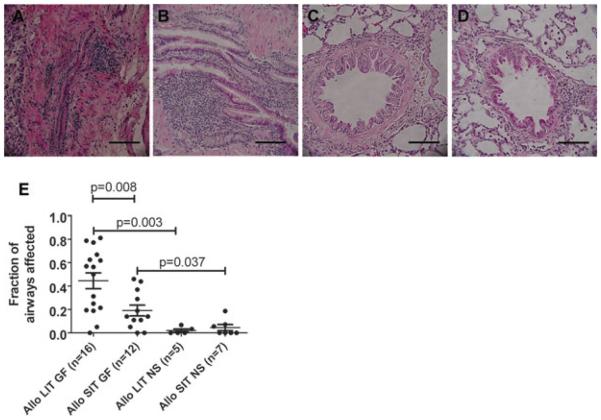
Aspiration of gastric fluid into the lung mediates the development of obliterative bronchiolitis (OB) in orthotopic WKY-to-F344 rat pulmonary transplants that have been subjected to immunosuppression with cyclosporine. However, the contribution of ischemic time to this process remains unknown. In this study, the effect of long (n = 16) and short (n = 12) ischemic times (average of 6 h and of 73 min, respectively) on rat lung transplants receiving aspiration of gastric fluid was assessed. Long ischemic times (LIT) led to significantly (p < 0.05) greater development of OB (ratio of OB lesions/total airways = 0.45 ± 0.07, mean ± standard error) compared to short ischemic times (ratio = 0.19 ± 0.05). However, the development of OB was dependent on aspiration, as controls receiving aspiration with normal saline showed little development of OB, regardless of ischemic time (p < 0.05). These data suggest that LIT, while insufficient by itself to lead to OB, works synergistically with aspiration of gastric fluid to exacerbate the development of OB.
© Copyright 2012 The American Society of Transplantation and the American Society of Transplant Surgeons.
Figures




References
-
- Annual Report of the U.S. Organ Procurement and Transplantation Network and the Scientific Registry of Transplant Recipients: Transplant Data 1999–2008. U.S. Dept of Health and Human Services; Rockville, MD: 2009.
-
- Belperio JA, Weigt SS, Fishbein MC, Lynch JP., 3rd Chronic lung allograft rejection: mechanisms and therapy. Proc Am Thorac Soc. 2009;6:108–121. - PubMed
-
- Stewart S, Fishbein MC, Snell GI, et al. Revision of the 1996 working formulation for the standardization of nomenclature in the diagnosis of lung rejection. J Heart Lung Transplant. 2007;26:1229–1242. - PubMed
-
- Sato M, Keshavjee S. Bronchiolitis obliterans syndrome: Alloimmune-dependent and -independent injury with aberrant tissue remodeling. Semin Thorac Cardiovasc Surg. 2008;20:173–182. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
