

Timing of progression from Chlamydia trachomatis infection to pelvic inflammatory disease: a mathematical modelling study
- PMID: 22883325
- PMCID: PMC3505463
- DOI: 10.1186/1471-2334-12-187
Timing of progression from Chlamydia trachomatis infection to pelvic inflammatory disease: a mathematical modelling study
Abstract
Background: Pelvic inflammatory disease (PID) results from the ascending spread of microorganisms from the vagina and endocervix to the upper genital tract. PID can lead to infertility, ectopic pregnancy and chronic pelvic pain. The timing of development of PID after the sexually transmitted bacterial infection Chlamydia trachomatis (chlamydia) might affect the impact of screening interventions, but is currently unknown. This study investigates three hypothetical processes for the timing of progression: at the start, at the end, or throughout the duration of chlamydia infection.
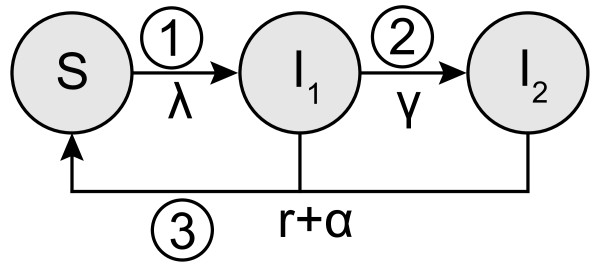
Methods: We develop a compartmental model that describes the trial structure of a published randomised controlled trial (RCT) and allows each of the three processes to be examined using the same model structure. The RCT estimated the effect of a single chlamydia screening test on the cumulative incidence of PID up to one year later. The fraction of chlamydia infected women who progress to PID is obtained for each hypothetical process by the maximum likelihood method using the results of the RCT.
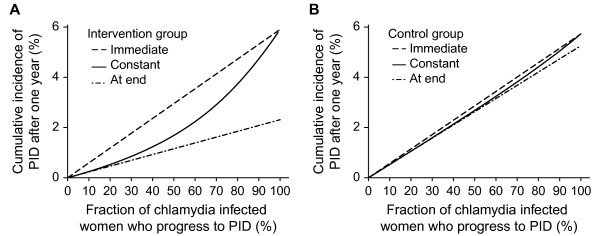
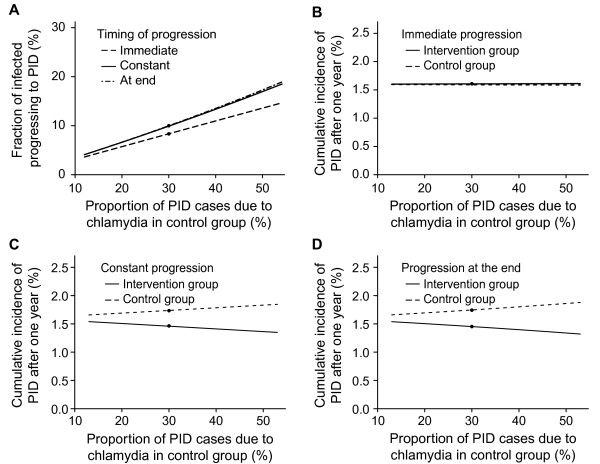
Results: The predicted cumulative incidence of PID cases from all causes after one year depends on the fraction of chlamydia infected women that progresses to PID and on the type of progression. Progression at a constant rate from a chlamydia infection to PID or at the end of the infection was compatible with the findings of the RCT. The corresponding estimated fraction of chlamydia infected women that develops PID is 10% (95% confidence interval 7-13%) in both processes.
Conclusions: The findings of this study suggest that clinical PID can occur throughout the course of a chlamydia infection, which will leave a window of opportunity for screening to prevent PID.
Figures
References
-
- Centers for Disease Control and Prevention. Case definitions for infectious conditions under public health surveillance. Centers for Disease Control and Prevention. MMWR Recomm Rep. 1997;46(RR-10):1–55. - PubMed
-
- Paavonen J, Westrom L, Eschenbach D. In: Sexually transmitted diseases. 4. Holmes KK, Sparling PF, Stamm W, Piot P, Wasserheit J, Corey L, Cohen M, editor. New York: McGraw-Hill Medical; 2008. Pelvic Inflammatory Disease; pp. 1017–1050.
-
- Low N, Bender N, Nartey L, Shang A, Stephenson JM. Effectiveness of chlamydia screening: systematic review. Int J Epidemiol. 2009;38:435–448. - PubMed
-
- World Health Organization. Global Prevalence and Incidence of Selected Curable Sexually Transmitted Infections: Overview and Estimates. Geneva: World Health Organization; 2001.
-
- Stamm WE. In: Sexually transmitted diseases. 4. Holmes KK, Sparling PF, Stamm W, Piot P, Wasserheit J, Corey L, Cohen M, editor. New York: McGraw-Hill Medical; 2008. Chlamydia trachomatis Infection of the Adults; pp. 575–593.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
