

Outcomes and temporal trends among high-risk patients after lung transplantation in the United States
- PMID: 22885156
- PMCID: PMC4131870
- DOI: 10.1016/j.healun.2012.07.001
Outcomes and temporal trends among high-risk patients after lung transplantation in the United States
Abstract
Introduction: Although several studies have evaluated risk factors for death after lung transplantation (LTx), few studies have focused on the highest-risk recipients. We undertook this study to evaluate the effect of high lung allocation scores (LAS), ventilator support, and extracorporeal membrane oxygenation (ECMO) support on outcomes after LTx.
Methods: We retrospectively reviewed all LTx recipients in the United Network for Organ Sharing database. Primary stratification was by recipient acuity at the time of LTx. The 3 strata consisted of (1) recipients in the highest LAS quartile (LAS ≥ 48.4), (2) those requiring ventilator support, and (3) those requiring ECMO support. The primary outcome was 1-year mortality. Sub-group analysis focused on temporal trends.
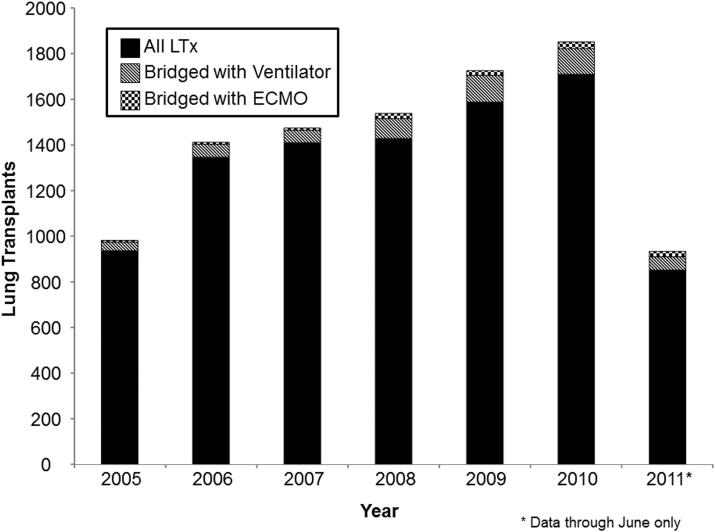
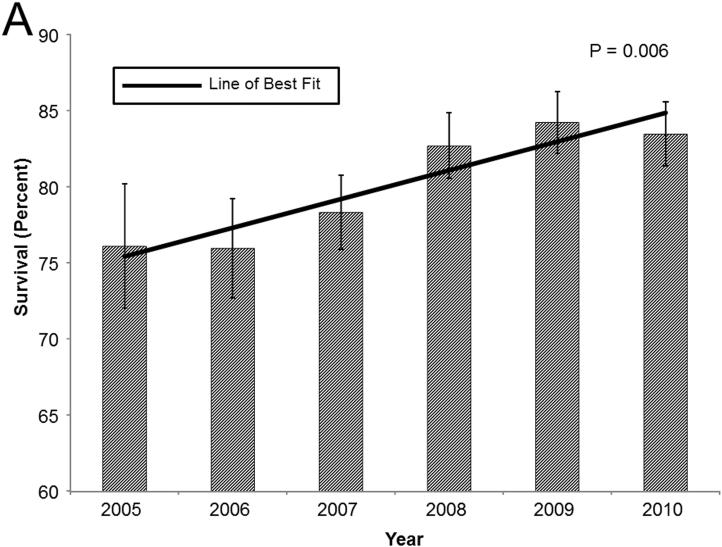
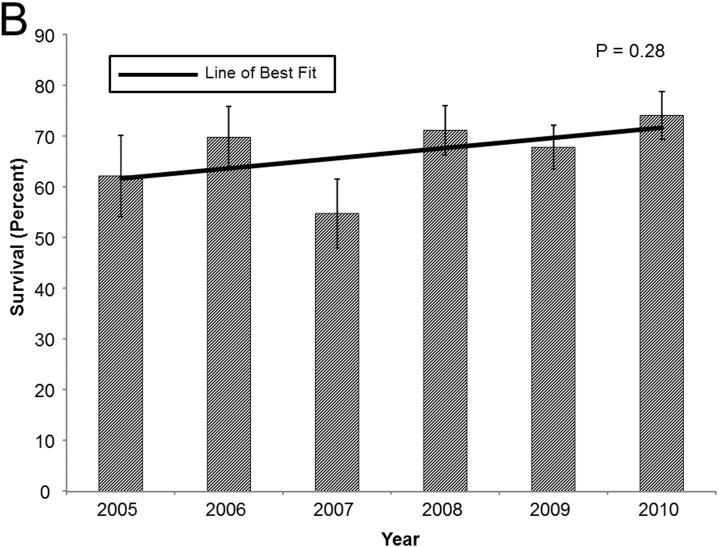
Results: From May 2005 to June 2011, 9,267 adults underwent LTx. Before LTx, 1,874 (20.2%) were in the highest LAS quartile, 526 (5.7%) required ventilator support, and 122 (1.3%) required ECMO support. Unadjusted analysis showed decreased 1-year survival associated with ventilator (67.7%) and ECMO support (57.6%) compared with the highest LAS quartile (81.0%; p < 0.001 for each comparison). These differences persisted on adjusted analysis for ventilator support (hazard ratio, 1.99, p < 0.001) and ECMO support (hazard ratio, 3.03; p < 0.001). Increasing annual center volume was associated with decreased mortality. In patients bridged to LTx with ECMO support, 1-year survival improved over time (coefficient, 8.03% per year; p = 0.06).
Conclusions: High-acuity LTx recipients, particularly those bridged with ventilator or ECMO support, have increased short-term mortality after LTx. However, since the introduction of the LAS, high-risk patients have demonstrated improving outcomes, particularly at high-volume centers.
Copyright © 2012. Published by Elsevier Inc.
Figures






References
-
- Egan TM, Murray S, Bustami RT, et al. Development of the new lung allocation system in the United States. Am J Transplant. 2006;6(5):1212–27. Pt 2. - PubMed
-
- Mason DP, Thuita L, Nowicki ER, et al. Should lung transplantation be performed for patients on mechanical respiratory support? The US experience. J Thorac Cardiovasc Surg. 2010;139(3):765–73. e1. - PubMed
-
- Bermudez CA, Rocha RV, Zaldonis D, et al. Extracorporeal membrane oxygenation as a bridge to lung transplant: midterm outcomes. Ann Thorac Surg. 2011;92(4):1226–31. discussion 31-2. - PubMed
-
- Vermeijden JW, Zijlstra JG, Erasmus ME, van der Bij W, Verschuuren EA. Lung transplantation for ventilator-dependent respiratory failure. J Heart Lung Transplant. 2009;28(4):347–51. - PubMed
-
- Bartz RR, Love RB, Leverson GE, et al. Pre-transplant mechanical ventilation and outcome in patients with cystic fibrosis. J Heart Lung Transplant. 2003;22(4):433–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
