

ICMR's tryst with HIV epidemic in India: 1986-1991
- PMID: 22885259
- PMCID: PMC3461712
ICMR's tryst with HIV epidemic in India: 1986-1991
Erratum in
-
Erratum.Indian J Med Res. 2012 Oct;136(4):687. Indian J Med Res. 2012. PMID: 31063285 Free PMC article. No abstract available.
Abstract
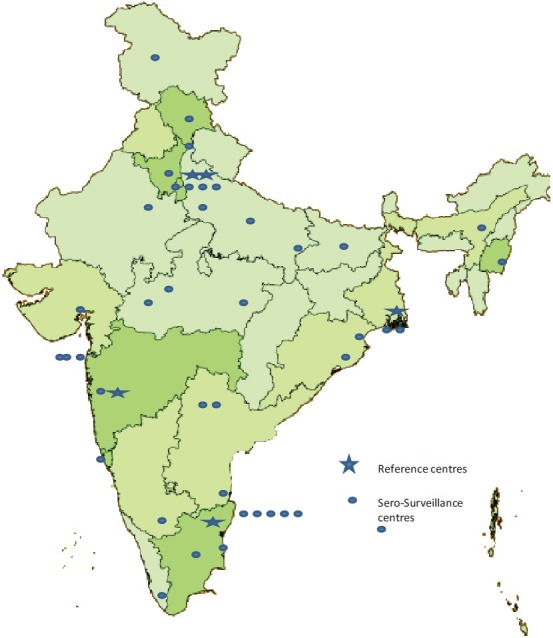
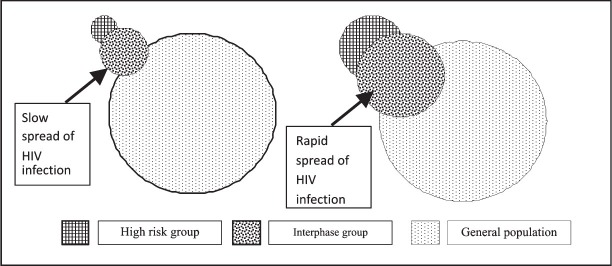
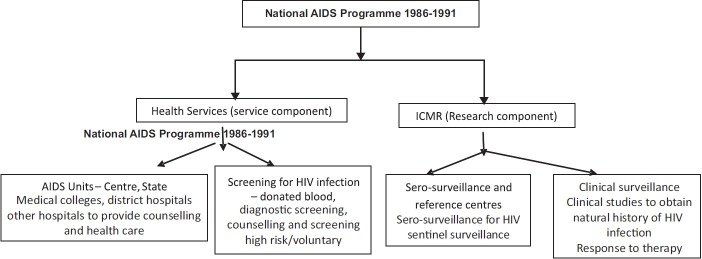
The Indian Council of Medical Research (ICMR) undertook screening of asymptomatic persons from high risk group with the ELISA test for HIV infection in 1986 and found that HIV infection has reached India. ICMR in collaboration with the central and State health services initiated the national sero-surveillance programme for HIV infection in 43 surveillance and five reference centres to determine the major modes of transmission and magnitude of infection. Data from the sero-surveillance showed that HIV infection was present in all the known high risk groups and in the general population in all the States both in urban and rural areas. HIV was getting transmitted through all the known modes of transmission. In most States heterosexual transmission was predominant but in Manipur intravenous (iv) drug use was the most common mode of transmission. Prevalence of HIV infection in high risk groups was not high and that in low risk groups was quite low. ICMR initiated hospital based sentinel surveillance in high risk groups and general population to obtain time trends in seroprevalence. Between 1986 and 1991, National AIDS Programme was carried out as a collaborative effort of ICMR, and central and State health services. As the dimensions of the epidemic unfolded, rational evidence based interventions which could be implemented within the existing health system, were initiated. National AIDS Control Programme (NACP) continued and upscaled all these interventions. Effective implementation of a multi-pronged, rational strategy for HIV infection containment and control right from the initial stages, and dedicated work done by committed professionals belonging to government and voluntary sectors, cultural ethos of the country, responsible behaviour of the population and relatively low iv drug use have resulted in rapid decline in new infection and in prevalence of infection within a quarter of a century after the initial detection of HIV.
Figures
References
-
- Centers for Disease Control (CDC) A cluster of Kaposi's sarcoma and Pneumocystis carinii pneumonia among homosexual male residents of Los Angeles and Orange Counties, California. MMWR Morb Mortal Wkly Rep. 1982;31:305–7. - PubMed
-
- Serwadda D, Mugerwa RD, Sewankambo NK, Lwegaba A, Carswell JW, Kirya GB, et al. Slim disease: a new disease in Uganda and its association with HTLV-III infection. Lancet. 1985;2:849–52. - PubMed
-
- Barre-Sinoussi F, Chermann JC, Rey F, Nugeyre MT, Chamaret S, Gruest J, et al. Isolation of a T-lymphotropic retrovirus from a patient at risk for acquired immune deficiency syndrome (AIDS) Science. 1983;220:868–71. - PubMed
-
- Kamradt T, Niese D, Vogel F. Slim disease (AIDS) Lancet. 1985;ii:1425. - PubMed
-
- Mann JM. AIDS: A worldwide pandemic. In: Gottlieb MS, Jeffries DF, Mildvan D, Pinching AJ, Quinn TC, Weiss RA, editors. Current topics in AIDS. Vol. 2. Chichester: John Wiley & Sons; 1989.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials