

Patient-centred assessment of COPD in primary care: experience from a cross-sectional study of health-related quality of life in Europe
- PMID: 22885563
- PMCID: PMC6547962
- DOI: 10.4104/pcrj.2012.00065
Patient-centred assessment of COPD in primary care: experience from a cross-sectional study of health-related quality of life in Europe
Abstract
Background: Most patients with chronic obstructive pulmonary disease (COPD) in Europe are treated in primary care, but perceptions on what guides primary care physicians (PCPs) in managing patients are lacking.
Aims: To describe factors associated with the assessment by PCPs of COPD severity and those associated with impaired health status, as assessed by patient-reported outcomes.
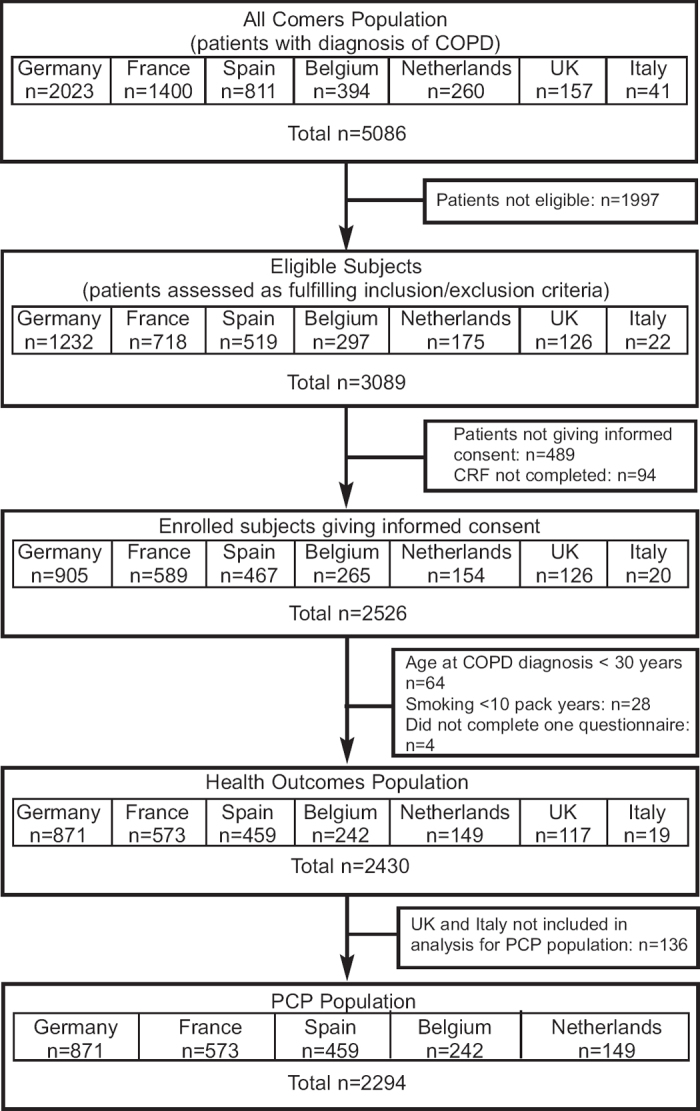
Methods: This cross-sectional study evaluated health-related quality of life (HRQL) in 2,294 COPD patients from five European countries. The severity of COPD was clinically judged by the PCPs and GOLD stage severity was calculated using spirometry data.
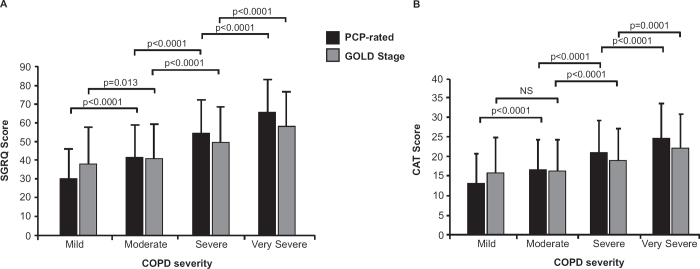
Results: PCPs' categories of severity reflected a wider range of HRQL scores (St George's Respiratory Questionnaire (SGRQ) total score: mild 30.3; moderate 41.7; severe 55.0; very severe 66.1) than GOLD severity grading (Stage I 38.2; Stage II 41.1; Stage III 49.9; Stage IV 58.5). Multiple ordinal logistic regression models showed that factors most closely related to PCP-rated COPD severity were Medical Research Council (MRC) dyspnoea grade, forced expiratory volume in 1 second (FEV₁) percent predicted, HRQL score (either SGRQ or COPD Assessment Test (CAT)), and previous hospitalisations (model generalised R²=0.45 or 0.44 (SQRQ or CAT in model, respectively); all factors p<0.0001). Factors with the highest association with HRQL scores (SGRQ or CAT) were MRC dyspnoea grade, COPD severity (PCP-rated), sputum production, and number of co-morbidities (model R²=0.46 or 0.37 (SQRQ or CAT in multiple linear regression model, respectively); all factors p<0.0001).
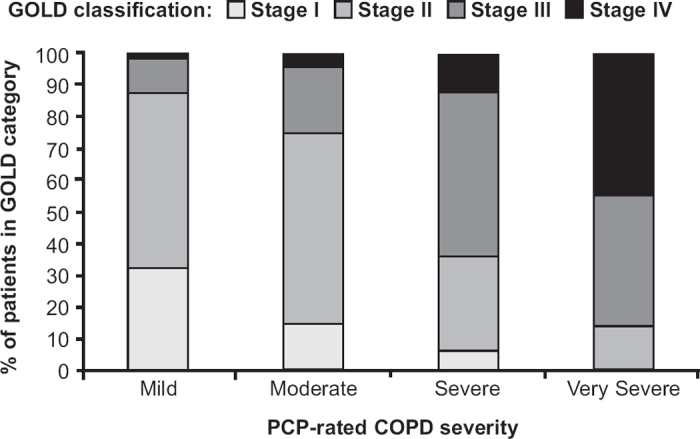
Conclusions: PCPs successfully graded COPD severity clinically and appeared to have greater discriminative power for assessing severity in COPD than FEV₁-based staging. Their more holistic approach appeared to reflect the patients' HRQL rating and was consistent across five European countries.
Conflict of interest statement
PWJ has received fees from pharmaceutical companies including GSK for speaking at meetings, participating in advisory board meetings, and to support research. GB has received honoraria for lectures and has participated in advisory board meetings for various pharmaceutical companies including GSK. PK has received lecture fees and participated in advisory boards and sponsored clinical trials for various pharmaceutical companies including GSK. MLL has served on advisory boards and received sponsorship, lecture fees and research funds from various pharmaceutical companies including GSK. JJSC has received lecture fees and research support from various pharmaceutical companies including GSK. LA and NB are employees of GSK. RWDN, TP and TvdM have no conflicts of interest to declare.
Figures
References
-
- Chapman KR, Mannino DM, Soriano JB, et al. Epidemiology and costs of chronic obstructive pulmonary disease. Eur Respir J 2006;27:188–207. http://dx.doi.org/10.1183/09031936.06.00024505 - PubMed
-
- The Global Initiative for Chronic Obstructive Lung disease (GOLD) revised 2009; www.goldcopd.com.
-
- Bellamy D, Bouchard J, Henrichsen S, et al. International Primary Care Respiratory Group (IPCRG) guidelines: management of chronic obstructive pulmonary disease (COPD). Prim Care Respir J 2006;15:48–57. http://dx.doi.org/10.1016/j.pcrj.2005.11.003 - PMC - PubMed
-
- Sobradillo-Pena V, Miravitlles M, Gabriel R, et al. Geographic variations in prevalence and underdiagnosis of COPD: results of the IBERPOC multicentre epidemiological study. Chest 2000;118:981–9. http://dx.doi.org/10.1378/chest.118.4.981 - PubMed
-
- Frank TL, Hazell ML, Linehan MF, Morris JA, Frank PI. The estimated prevalence of chronic obstructive pulmonary disease in a general practice population. Prim Care Respir J 2007;16:169–73. http://dx.doi.org/10.3132/pcrj.2007.00028 - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous