

Shortened surveillance intervals following suboptimal bowel preparation for colonoscopy: results of a national survey
- PMID: 22885884
- PMCID: PMC3561457
- DOI: 10.1007/s00384-012-1559-7
Shortened surveillance intervals following suboptimal bowel preparation for colonoscopy: results of a national survey
Abstract
Purpose: Suboptimal bowel preparation can result in decreased neoplasia detection, shortened surveillance intervals, and increased costs. We assessed bowel preparation recommendations and the relationship to self-reported proportion of suboptimal bowel preparations in practice; and evaluated the impact of suboptimal bowel preparation on colonoscopy surveillance practices. A random sample of a national organization of gastroenterologists in the U.S. was surveyed.
Methods: Demographic and practice characteristics, bowel preparation regimens, and proportion of suboptimal bowel preparations in practice were ascertained. Recommended follow-up colonoscopy intervals were evaluated for optimal and suboptimal bowel preparation and select clinical scenarios.
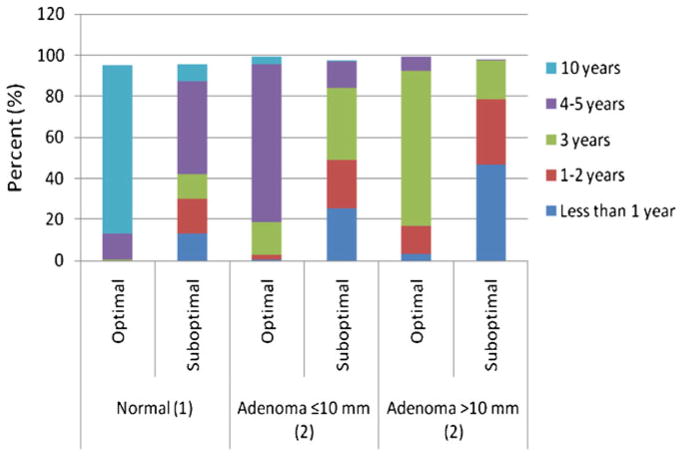
Results: We identified 6,777 physicians, of which 1,354 were randomly selected; 999 were eligible, and 288 completed the survey. Higher proportion of suboptimal bowel preparations/week (≥10 %) was associated with hospital/university practice, teaching hospital affiliation, >25 % Medicaid insured patients, recommendation of PEG alone and sulfate-free. Those reporting >25 % Medicare and privately insured patients, split dose recommendation, and use of MoviPrep® were associated with a <10 % suboptimal bowel preparations/week. Shorter surveillance intervals for three clinical scenarios were reported for suboptimal preparations and were shortest among participants in the Northeast who more often recommended early follow-up for normal findings and small adenomas. Those who recommended 4-l PEG alone more often advised <1 year surveillance interval for a large adenoma.
Conclusions: Our study demonstrates significantly shortened surveillance interval recommendations for suboptimal bowel preparation and that these interval recommendations vary regionally in the United States. Findings suggest an interrelationship between dietary restriction, purgative type, and practice and patient characteristics that warrant additional research.
Conflict of interest statement
Figures
References
-
- American Cancer Society. Colorectal cancer facts and figures, 2011–2013. American Cancer Society; Atlanta: 2011.
-
- Levin B, Lieberman DA, McFarland B, Smith RA, Brooks D, Andrews KS, et al. Screening and surveillance for the early detection of colorectal cancer and adenomatous polyps, 2008: a joint guideline from the American Cancer Society, the US Multi-Society Task Force on Colorectal Cancer, and the American College of Radiology. CA Cancer J Clin. 2008;58:130–160. - PubMed
-
- Rex DK, Johnson DA, Lieberman DA, Burt RW, Sonnenberg A. Colorectal cancer prevention 2000: screening recommendations of the American College of Gastroenterology. Am J Gastroenterol. 2000;95:868–877. - PubMed
-
- Lieberman DA, Holub J, Eisen G, Kraemer D, Morris CD. Utilization of colonoscopy in the United States: results from a national consortium. Gastrointest Endosc. 2005;62:875–883. - PubMed
-
- Lieberman DA, De Garmo PL, Fleischer DE, Eisen GM, Helfand M. Patterns of endoscopy use in the United States. Gastroenterol. 2000;118:619–624. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
