

β-Arrestin-biased AT1R stimulation promotes cell survival during acute cardiac injury
- PMID: 22886417
- PMCID: PMC3469643
- DOI: 10.1152/ajpheart.00475.2012
β-Arrestin-biased AT1R stimulation promotes cell survival during acute cardiac injury
Abstract
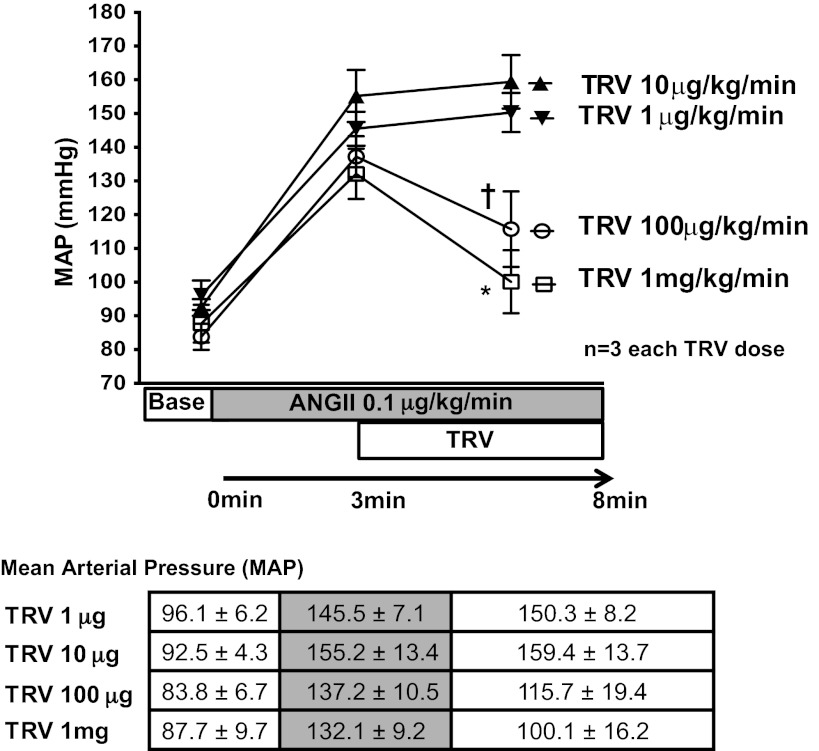
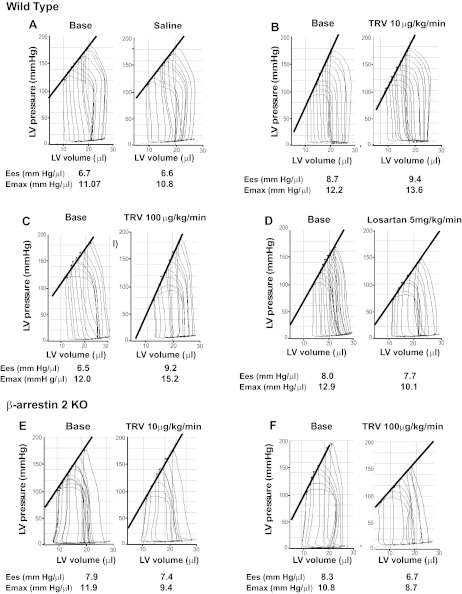
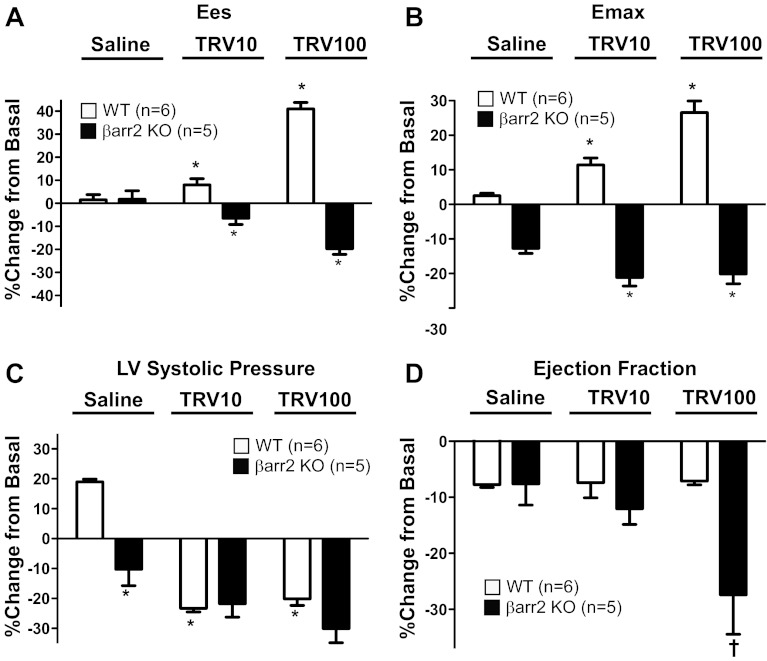
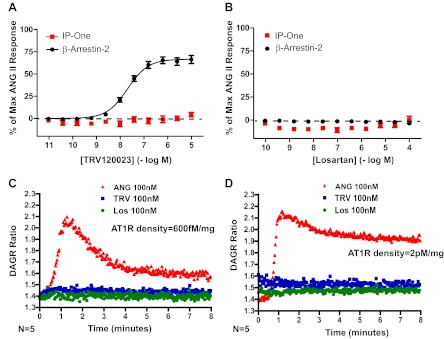
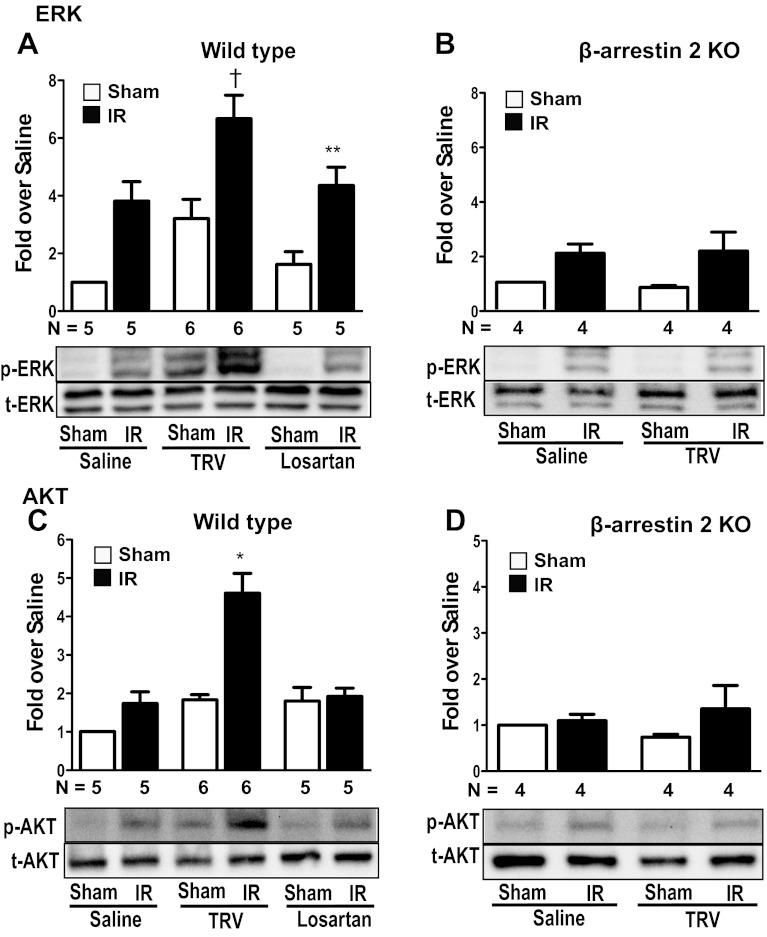
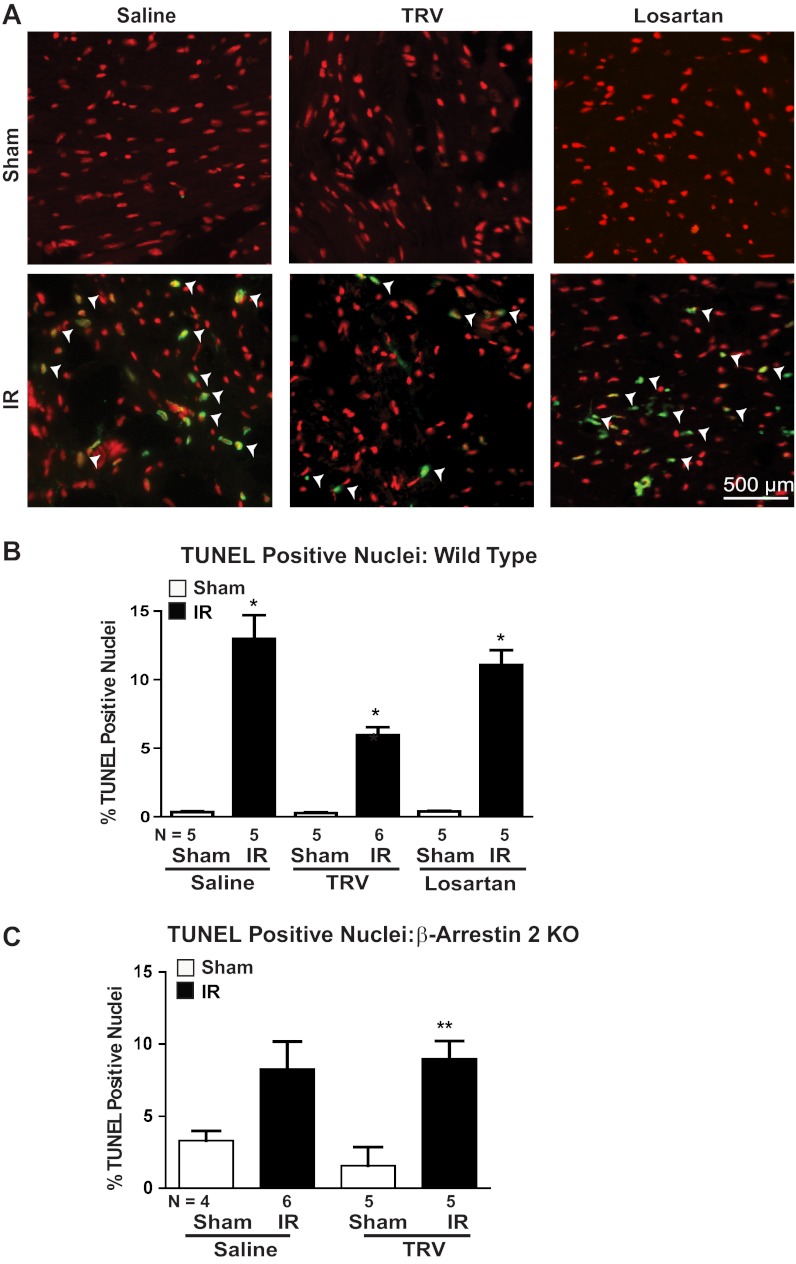
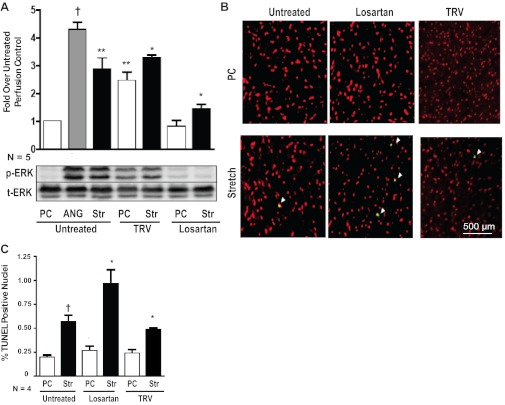
Pharmacological blockade of the ANG II type 1 receptor (AT1R) is a common therapy for treatment of congestive heart failure and hypertension. Increasing evidence suggests that selective engagement of β-arrestin-mediated AT1R signaling, referred to as biased signaling, promotes cardioprotective signaling. Here, we tested the hypothesis that a β-arrestin-biased AT1R ligand TRV120023 would confer cardioprotection in response to acute cardiac injury compared with the traditional AT1R blocker (ARB), losartan. TRV120023 promotes cardiac contractility, assessed by pressure-volume loop analyses, while blocking the effects of endogenous ANG II. Compared with losartan, TRV120023 significantly activates MAPK and Akt signaling pathways. These hemodynamic and biochemical effects were lost in β-arrestin-2 knockout (KO) mice. In response to cardiac injury induced by ischemia reperfusion injury or mechanical stretch, pretreatment with TRV120023 significantly diminishes cell death compared with losartan, which did not appear to be cardioprotective. This cytoprotective effect was lost in β-arrestin-2 KO mice. The β-arrestin-biased AT1R ligand, TRV120023, has cardioprotective and functional properties in vivo, which are distinct from losartan. Our data suggest that this novel class of drugs may provide an advantage over conventional ARBs by supporting cardiac function and reducing cellular injury during acute cardiac injury.
Figures
References
-
- Effect of enalapril on mortality and the development of heart failure in asymptomatic patients with reduced left ventricular ejection fractions. The SOLVD Investigators. N Engl J Med 327: 685–691, 1992 - PubMed
-
- Effect of enalapril on survival in patients with reduced left ventricular ejection fractions and congestive heart failure. The SOLVD Investigators. N Engl J Med 325: 293–302, 1991 - PubMed
-
- Ahn S, Shenoy SK, Wei H, Lefkowitz RJ. Differential kinetic and spatial patterns of beta-arrestin and G protein-mediated ERK1/2 activation by the angiotensin II receptor. J Biol Chem 279: 35518–35525, 2004 - PubMed
-
- Ainscough JF, Drinkhill MJ, Sedo A, Turner NA, Brooke DA, Balmforth AJ, Ball SG. Angiotensin II type-1 receptor activation in the adult heart causes blood pressure-independent hypertrophy and cardiac dysfunction. Cardiovasc Res 81: 592–600, 2009 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Research Materials
Miscellaneous