

Sex differences in clinical characteristics and outcomes in elderly patients with heart failure and preserved ejection fraction: the Irbesartan in Heart Failure with Preserved Ejection Fraction (I-PRESERVE) trial
- PMID: 22887722
- PMCID: PMC4768740
- DOI: 10.1161/CIRCHEARTFAILURE.112.970061
Sex differences in clinical characteristics and outcomes in elderly patients with heart failure and preserved ejection fraction: the Irbesartan in Heart Failure with Preserved Ejection Fraction (I-PRESERVE) trial
Abstract
Background: There are few sex-specific outcome data in heart failure with preserved ejection fraction.
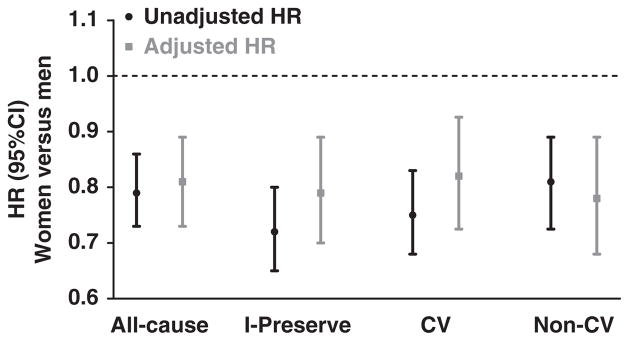
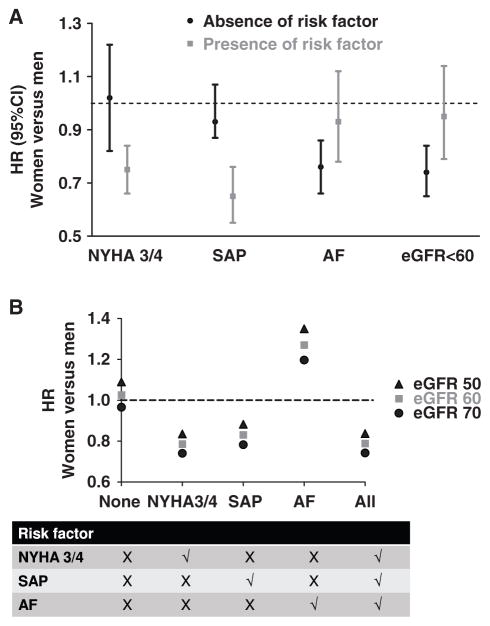
Methods and results: We assessed sex differences in baseline characteristics and outcomes among 4128 patients with heart failure with preserved ejection fraction in the Irbesartan in Heart Failure with Preserved Ejection Fraction (I-PRESERVE) trial. Women (n=2491) with heart failure with preserved ejection fraction were ≈1 year older (72±7 years versus 71±7 years) and more likely to be obese (46% versus 35%) and have chronic kidney disease (34% versus 26%) and hypertension (91% versus 85%) than men but less likely to have an ischemic cause (19% versus 34%), atrial fibrillation (27% versus 33%), or chronic obstructive pulmonary disease (8% versus 13%) (all P<0.001). During a mean of 49.5 months, there were 881 deaths (447 in women, 434 in men; risk ratio, 0.64; 95% CI, 0.56-0.74) and 5776 hospitalizations (3239 in women, 2537 in men; risk ratio, 0.80; 95% CI, 0.76-0.84). Women had lower risk of all-cause events (deaths and hospitalizations), even after adjusting for baseline characteristics (adjusted hazards ratio, 0.81; 95% CI, 0.73-0.89). However, the sex-related difference in risk of all-cause events was modified in the presence or absence of atrial fibrillation, renal dysfunction, stable angina pectoris, or advanced New York Heart Association class symptoms.
Conclusions: In patients with typical heart failure with preserved ejection fraction, there were prominent sex differences in baseline characteristics and outcomes. Women had better overall prognosis, although the presence of 4 common baseline characteristics seemed to moderate this finding.
Trial registration: ClinicalTrials.gov NCT00095238.
Figures
References
-
- Kitzman DW, Gardin JM, Gottdiener JS, Arnold A, Boineau R, Aurigemma G, Marino EK, Lyles M, Cushman M, Enright PL Cardiovascular Health Study Research Group. Importance of heart failure with preserved systolic function in patients > or = 65 years of age. CHS Research Group. Cardiovascular Health Study. Am J Cardiol. 2001;87:413–419. - PubMed
-
- Vasan RS, Larson MG, Benjamin EJ, Evans JC, Reiss CK, Levy D. Congestive heart failure in subjects with normal versus reduced left ventricular ejection fraction: prevalence and mortality in a population-based cohort. J Am Coll Cardiol. 1999;33:1948–1955. - PubMed
-
- Devereux RB, Roman MJ, Liu JE, Welty TK, Lee ET, Rodeheffer R, Fabsitz RR, Howard BV. Congestive heart failure despite normal left ventricular systolic function in a population-based sample: the Strong Heart Study. Am J Cardiol. 2000;86:1090–1096. - PubMed
-
- Kupari M, Lindroos M, Iivanainen AM, Heikkilä J, Tilvis R. Congestive heart failure in old age: prevalence, mechanisms and 4-year prognosis in the Helsinki Ageing Study. J Intern Med. 1997;241:387–394. - PubMed
-
- Masoudi FA, Havranek EP, Smith G, Fish RH, Steiner JF, Ordin DL, Krumholz HM. Gender, age, and heart failure with preserved left ventricular systolic function. J Am Coll Cardiol. 2003;41:217–223. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
