

Weight loss after sleeve gastrectomy in super superobesity
- PMID: 22888410
- PMCID: PMC3409558
- DOI: 10.1155/2012/959260
Weight loss after sleeve gastrectomy in super superobesity
Abstract
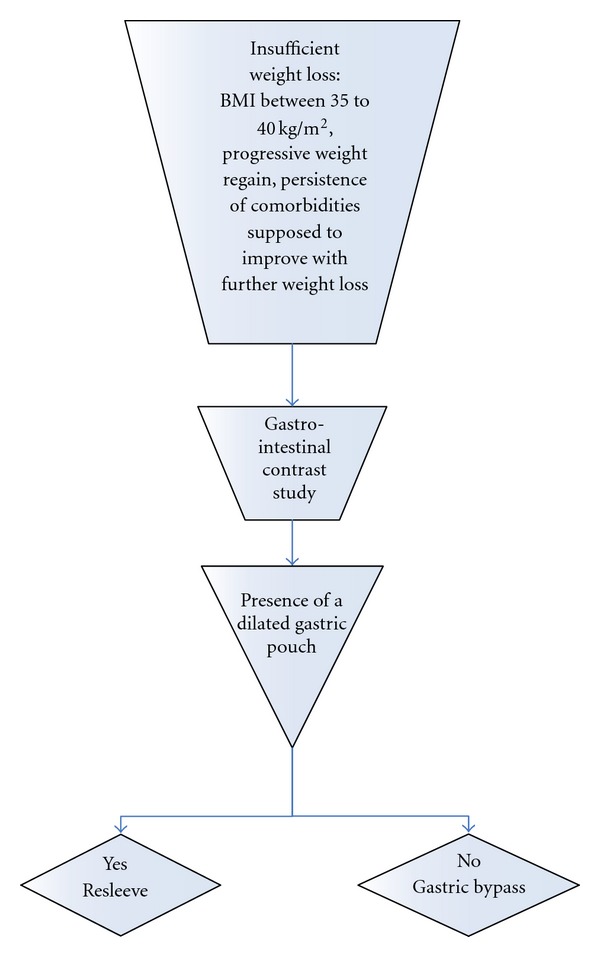
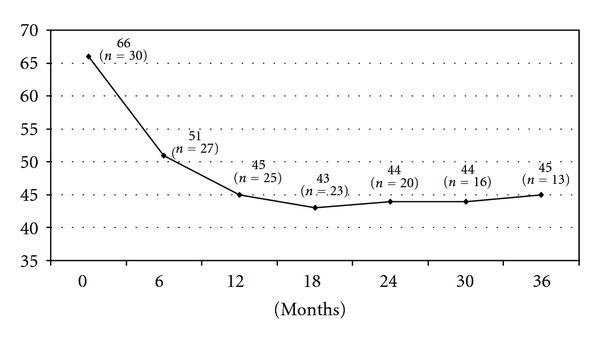
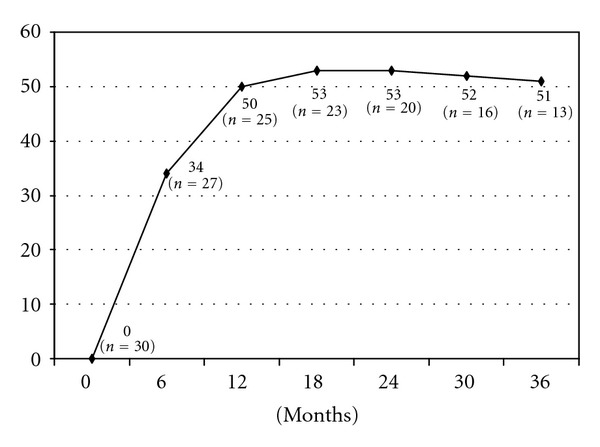
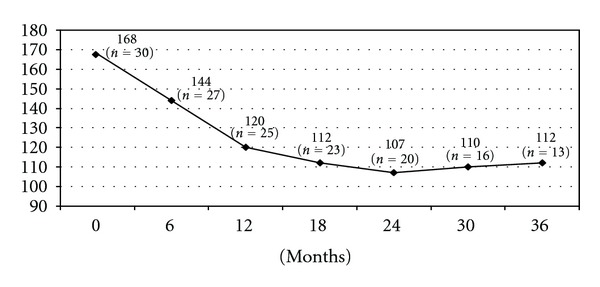
Objective. This prospective study evaluated laparoscopic sleeve gastrectomy for its safety and efficiency in excess weight loss (%EWL) in super superobese patients (BMI >60 Kg/m(2)). Results. Thirty patients (33 women and 7 men) were included, with mean age of 35 years (range 18 to 59). Mean preoperative BMI was 66 Kg/m(2) (range 60 to 85). The study included one patient with complete situs inversus and 4 (14%) with previous restrictive gastric banding. The mean operative time was 120 minutes (range 80 to 220 min) and the mean hospital stay was 7.5 days (4 to 28 days). There was no postoperative mortality or need for a laparotomy conversion. Two subphrenic hematomas, one gastric fistula, and one pulmonary embolism, were the major complications. After 18 months 17 (77%) had sufficient weight loss and six had insufficient results, leading to either re-sleeve gastrectomy (3), or gastric bypass (2). Three years after the initial laparoscopic sleeve gastrectomy, the mean EWL was 51% (range 21 to 82). Conclusion. The laparoscopic sleeve gastrectomy is a safe and efficient operating procedure for treating super superobesity. In the case of insufficient weight loss, a second-stage operation like resleeve gastrectomy or gastric bypass can be proposed.
Figures
Similar articles
-
Heterogeneity of weight loss after gastric bypass, sleeve gastrectomy, and adjustable gastric banding.Surgery. 2019 Mar;165(3):565-570. doi: 10.1016/j.surg.2018.08.023. Epub 2018 Oct 11. Surgery. 2019. PMID: 30316577
-
Laparoscopic sleeve gastrectomy followed by duodenal switch in selected patients versus single-stage duodenal switch for superobesity: case-control study.Surg Obes Relat Dis. 2013 Jul-Aug;9(4):531-8. doi: 10.1016/j.soard.2012.02.003. Epub 2012 Mar 3. Surg Obes Relat Dis. 2013. PMID: 22498357
-
Results of laparoscopic sleeve gastrectomy: a prospective study in 135 patients with morbid obesity.Surgery. 2009 Jan;145(1):106-13. doi: 10.1016/j.surg.2008.07.013. Epub 2008 Sep 30. Surgery. 2009. PMID: 19081482
-
Safety and Outcome of Laparoscopic Sleeve Gastrectomy Following Removal of Adjustable Gastric Banding: Lessons from 109 Patients in a Single Center and Review of the Literature.Obes Surg. 2017 May;27(5):1266-1270. doi: 10.1007/s11695-016-2463-y. Obes Surg. 2017. PMID: 27885536 Review.
-
Resleeve for failed laparoscopic sleeve gastrectomy: systematic review and meta-analysis.Surg Obes Relat Dis. 2020 Oct;16(10):1383-1391. doi: 10.1016/j.soard.2020.06.007. Epub 2020 Jun 11. Surg Obes Relat Dis. 2020. PMID: 32682774
Cited by
-
The advantages and disadvantages of sleeve gastrectomy; clinical laboratory to bedside review.Heliyon. 2020 Feb 29;6(2):e03496. doi: 10.1016/j.heliyon.2020.e03496. eCollection 2020 Feb. Heliyon. 2020. PMID: 32154399 Free PMC article. Review.
-
The first survey addressing patients with BMI over 50: a survey of 789 bariatric surgeons.Surg Endosc. 2022 Aug;36(8):6170-6180. doi: 10.1007/s00464-021-08979-w. Epub 2022 Jan 21. Surg Endosc. 2022. PMID: 35064321 Free PMC article.
-
Comparison of laparoscopic sleeve gastrectomy leak rates in five staple-line reinforcement options: a systematic review.Surg Endosc. 2020 Jan;34(1):396-407. doi: 10.1007/s00464-019-06782-2. Epub 2019 Apr 16. Surg Endosc. 2020. PMID: 30993513 Free PMC article.
-
One anastomosis gastric bypass as a one-stage bariatric surgical procedure in patients with BMI ≥ 50 kg/m2.Sci Rep. 2022 Jun 22;12(1):10507. doi: 10.1038/s41598-022-14485-3. Sci Rep. 2022. PMID: 35732861 Free PMC article.
-
Scientific Evidence for the Updated Guidelines on Indications for Metabolic and Bariatric Surgery (IFSO/ASMBS).Obes Surg. 2024 Nov;34(11):3963-4096. doi: 10.1007/s11695-024-07370-7. Epub 2024 Sep 25. Obes Surg. 2024. PMID: 39320627 Free PMC article.
References
-
- Dresel A, Kuhn JA, McCarty TM. Laparoscopic Roux-en-Y gastric bypass in morbidly obese and super morbidly obese patients. American Journal of Surgery. 2004;187(2):230–232. - PubMed
-
- Regan JP, Inabnet WB, Gagner M, Pomp A. Early experience with two-stage laparoscopic Roux-en-Y gastric bypass as an alternative in the super-super obese patient. Obesity Surgery. 2003;13(6):861–864. - PubMed
-
- Catheline JM, Fysekidis M, Bihan H, Boschetto A, Dbouk R, et al. Better results in weight loss after the second gastrectomy in re-sleeve gastrectomy. Journal of Obesity and Weight Loss Therapy. 2011;1, article 107
LinkOut - more resources
Full Text Sources
