

Prognostic utility and characterization of cell-free DNA in patients with severe sepsis
- PMID: 22889177
- PMCID: PMC3580740
- DOI: 10.1186/cc11466
Prognostic utility and characterization of cell-free DNA in patients with severe sepsis
Abstract
Introduction: Although sepsis is the leading cause of death in noncoronary critically ill patients, identification of patients at high risk of death remains a challenge. In this study, we examined the incremental usefulness of adding multiple biomarkers to clinical scoring systems for predicting intensive care unit (ICU) mortality in patients with severe sepsis.
Methods: This retrospective observational study used stored plasma samples obtained from 80 severe sepsis patients recruited at three tertiary hospital ICUs in Hamilton, Ontario, Canada. Clinical data and plasma samples were obtained at study inclusion for all 80 patients, and then daily for 1 week, and weekly thereafter for a subset of 50 patients. Plasma levels of cell-free DNA (cfDNA), interleukin 6 (IL-6), thrombin, and protein C were measured and compared with clinical characteristics, including the primary outcome of ICU mortality and morbidity measured with the Multiple Organ Dysfunction (MODS) score and Acute Physiology and Chronic Health Evaluation (APACHE) II scores.
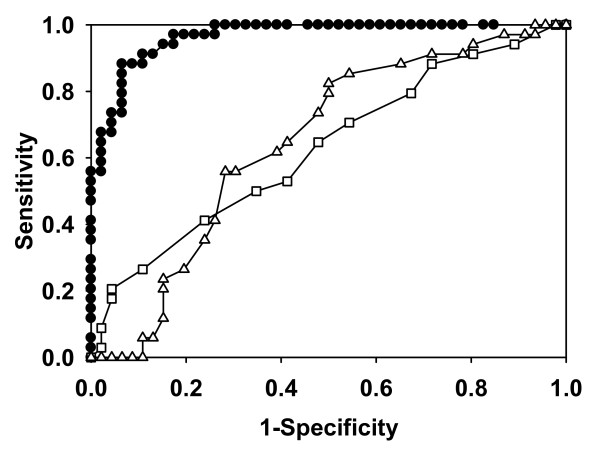
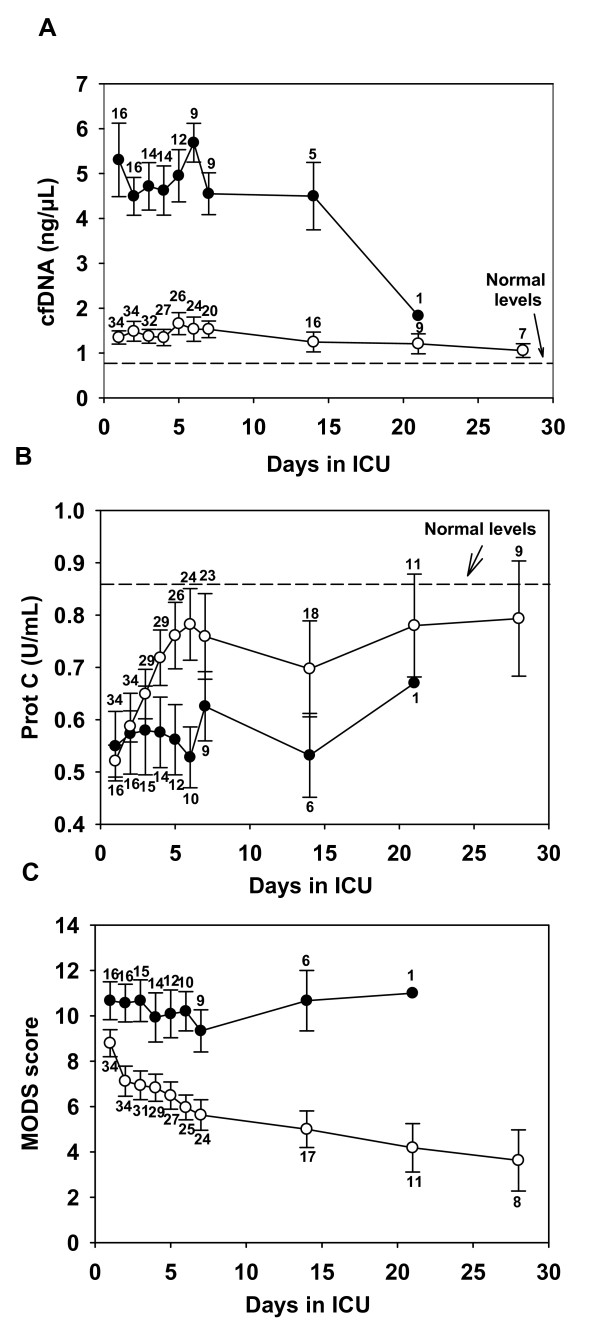
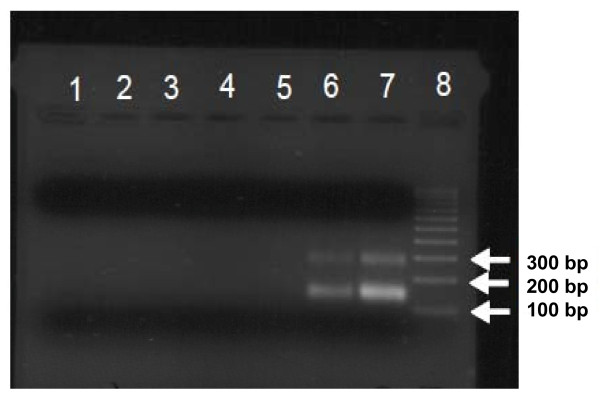
Results: The level of cfDNA in plasma at study inclusion had better prognostic utility than did MODS or APACHE II scores, or the biomarkers measured. The area under the receiver operating characteristic (ROC) curves for cfDNA to predict ICU mortality is 0.97 (95% CI, 0.93 to 1.00) and to predict hospital mortality is 0.84 (95% CI, 0.75 to 0.94). We found that a cfDNA cutoff value of 2.35 ng/μl had a sensitivity of 87.9% and specificity of 93.5% for predicting ICU mortality. Sequential measurements of cfDNA suggested that ICU mortality may be predicted within 24 hours of study inclusion, and that the predictive power of cfDNA may be enhanced by combining it with protein C levels or MODS scores. DNA-sequence analyses and studies with Toll-like receptor 9 (TLR9) reporter cells suggests that the cfDNA from sepsis patients is host derived.
Conclusions: These studies suggest that cfDNA provides high prognostic accuracy in patients with severe sepsis. The serial data suggest that the combination of cfDNA with protein C and MODS scores may yield even stronger predictive power. Incorporation of cfDNA in sepsis risk-stratification systems may be valuable for clinical decision making or for inclusion into sepsis trials.
Figures
Comment in
-
Cell-free DNA and outcome in sepsis.Crit Care. 2012 Nov 8;16(6):170. doi: 10.1186/cc11508. Crit Care. 2012. PMID: 23140420 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
