

Interleukin-6 is the strongest predictor of 30-day mortality in patients with cardiogenic shock due to myocardial infarction
- PMID: 22889197
- PMCID: PMC3580741
- DOI: 10.1186/cc11467
Interleukin-6 is the strongest predictor of 30-day mortality in patients with cardiogenic shock due to myocardial infarction
Abstract
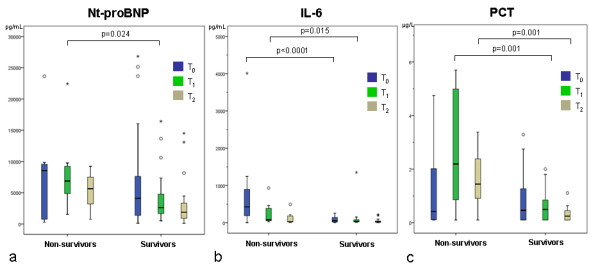
Introduction: Cardiogenic shock (CS) remains the leading cause of death in patients hospitalized for myocardial infarction (MI). Systemic inflammation with inappropriate vasodilatation is observed in many patients with CS and may contribute to an excess mortality rate. The purpose of this study was to determine the predictive role of serial measurements of Nt-proBNP, interleukin-6 (IL-6), and procalcitonin (PCT) for 30-day mortality in patients with CS due to MI.
Methods: The present study is a prospective single-center study including 87 patients with MI complicated by CS treated with acute revascularization and intraaortic balloon counterpulsation (IABP) support. Predictive values of plasma levels at admission (T0), after 24 hours (T1), and after 72 hours (T2) were examined according to 30-day mortality.
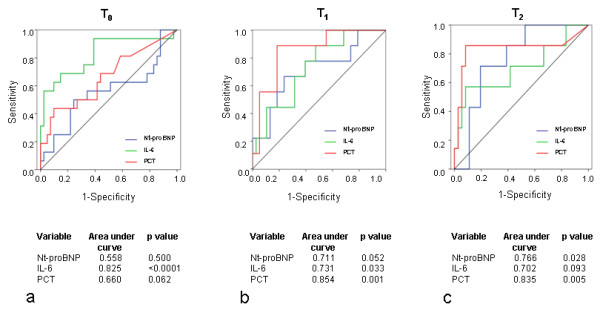
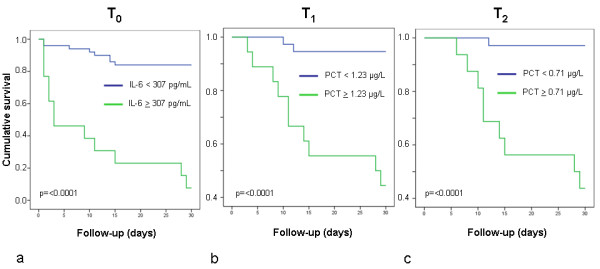
Results: Significant differences between survivors (n = 59) and nonsurvivors (n = 28) were seen for Nt-proBNP at T0, for IL-6 at T0 and T1, and for PCT at T1 and T2. According to ROC analyses, the highest accuracy predicting 30-day mortality was seen at T0 for IL-6, at T1 for PCT, and at T2 for PCT. In univariate analysis, significant values were found for Nt-proBNP at T1, and for IL-6 and PCT at all points in time. Within the multivariate analysis, age, creatinine, and IL-6 were significant determinants of 30-day mortality, in which IL-6 showed the highest level of significance.
Conclusions: In patients with MI complicated by CS, IL-6 represented a reliable independent early prognostic marker of 30-day mortality. PCT revealed a significant value at later points in time, whereas Nt-proBNP seemed to be of lower relevance.
Figures
References
-
- Goldberg RJ, Spencer FA, Gore JM, Lessard D, Yarzebski J. Thirty-year trends (1975 to 2005) in the magnitude of, management of, and hospital death rates associated with cardiogenic shock in patients with acute myocardial infarction: a population-based perspective. Circulation. 2009;119:1211–1219. doi: 10.1161/CIRCULATIONAHA.108.814947. - DOI - PMC - PubMed
-
- Hochman JS, Sleeper LA, White HD, Dzavik V, Wong SC, Menon V, Webb JG, Steingart R, Picard MH, Menegus MA, Boland J, Sanborn T, Buller CE, Modur S, Forman R, Desvigne-Nickens P, Jacobs AK, Slater JN, LeJemtel TH. SHOCK Investigators: Should We Emergently Revascularize Occluded Coronaries for Cardiogenic Shock: one-year survival following early revascularization for cardiogenic shock. JAMA. 2001;285:190–192. doi: 10.1001/jama.285.2.190. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
