

Vasopressin and terlipressin in adult vasodilatory shock: a systematic review and meta-analysis of nine randomized controlled trials
- PMID: 22889256
- PMCID: PMC3580743
- DOI: 10.1186/cc11469
Vasopressin and terlipressin in adult vasodilatory shock: a systematic review and meta-analysis of nine randomized controlled trials
Abstract
Introduction: Catecholamines are the most used vasopressors in vasodilatory shock. However, the development of adrenergic hyposensitivity and the subsequent loss of catecholamine pressor activity necessitate the search for other options. Our aim was to evaluate the effects of vasopressin and its analog terlipressin compared with catecholamine infusion alone in vasodilatory shock.
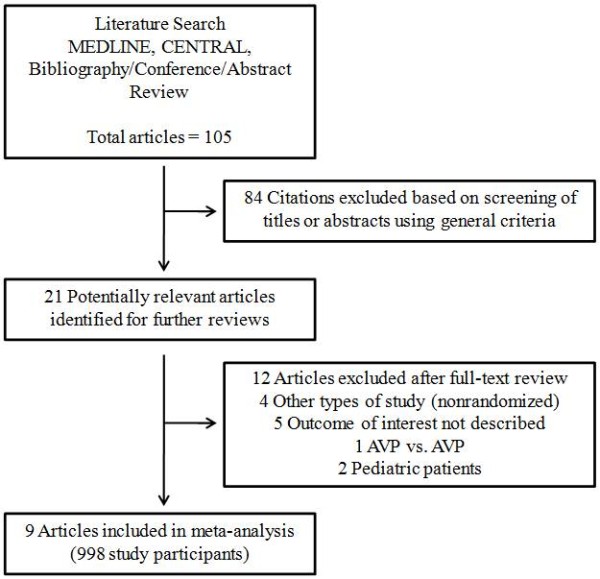
Methods: A systematic review and meta-analysis of publications between 1966 and 2011 was performed. The Medline and CENTRAL databases were searched for studies on vasopressin and terlipressin in critically ill patients. The meta-analysis was limited to randomized controlled trials evaluating the use of vasopressin and/or terlipressin compared with catecholamine in adult patients with vasodilatory shock. The assessed outcomes were: overall survival, changes in the hemodynamic and biochemical variables, a decrease of catecholamine requirements, and adverse events.
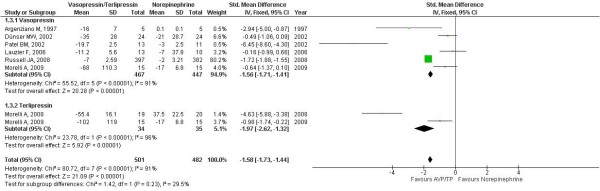
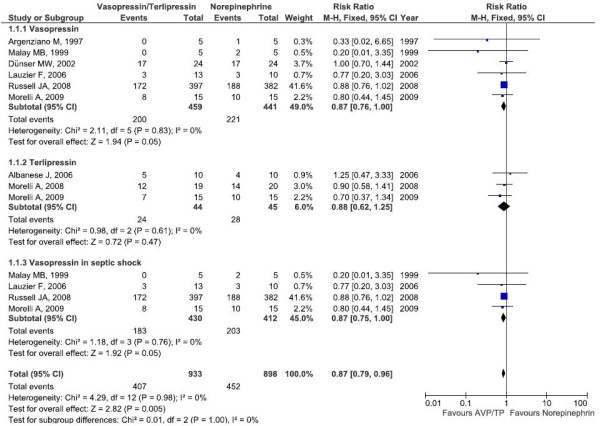
Results: Nine trials covering 998 participants were included. A meta-analysis using a fixed-effect model showed a reduction in norepinephrine requirement among patients receiving terlipressin or vasopressin infusion compared with control (standardized mean difference, -1.58 (95% confidence interval, -1.73 to -1.44); P < 0.0001). Overall, vasopressin and terlipressin, as compared with norepinephrine, reduced mortality (relative risk (RR), 0.87 (0.77 to 0.99); P = 0.04). Vasopressin compared with norepinephrine decreased mortality in adult patients (RR, 0.87 (0.76 to 1.00); P = 0.05) and in patients with septic shock (42.5% vs. 49.2%, respectively; RR, 0.87 (0.75 to 1.00); P = 0.05; number needed to treat, 1 to 15). There was no difference in adverse events between the vasopressin and control groups (RR, 0.98 (0.65 to 1.47); P = 0.92).
Conclusions: Vasopressin use in vasodilatory shock is safe, associated with reduced mortality, and facilitates weaning of catecholamines. In patients with septic shock, use of vasopressin compared with norepinephrine may also decrease mortality.
Figures
Comment in
-
Vasopressin and terlipressin in adult vasodilatory shock.Crit Care. 2012 Dec 28;16(6):470; author reply 470. doi: 10.1186/cc11887. Crit Care. 2012. PMID: 23273051 Free PMC article. No abstract available.
References
-
- Dellinger RP, Levy MM, Carlet JM, Bion J, Parker MM, Jaeschke R, Reinhart K, Angus DC, Brun-Buisson C, Beale R, Calandra T, Dhainaut JF, Gerlach H, Harvey M, Marini JJ, Marshall J, Ranieri M, Ramsay G, Sevransky J, Thompson BT, Townsend S, Vender JS, Zimmerman JL, Vincent JL. International Surviving Sepsis Campaign Guidelines Committee; American Association of Critical-Care Nurses; American College of Chest Physicians; American College of Emergency Physicians; Canadian Critical Care Society; European Society of Clinical Microbiology and Infectious Diseases et al. Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock: 2008. Crit Care Med. 2008;36:296–327. doi: 10.1097/01.CCM.0000298158.12101.41. - DOI - PubMed
-
- Mullner M, Urbanek B, Havel C, Losert H, Waechter F, Gamper G. Vasopressors for shock. Cochrane Database Syst Rev. 2004;3:CD003709. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
