

Lymphocytic choriomeningitis virus: an underrecognized cause of neurologic disease in the fetus, child, and adult
- PMID: 22889536
- PMCID: PMC4256959
- DOI: 10.1016/j.spen.2012.02.002
Lymphocytic choriomeningitis virus: an underrecognized cause of neurologic disease in the fetus, child, and adult
Abstract
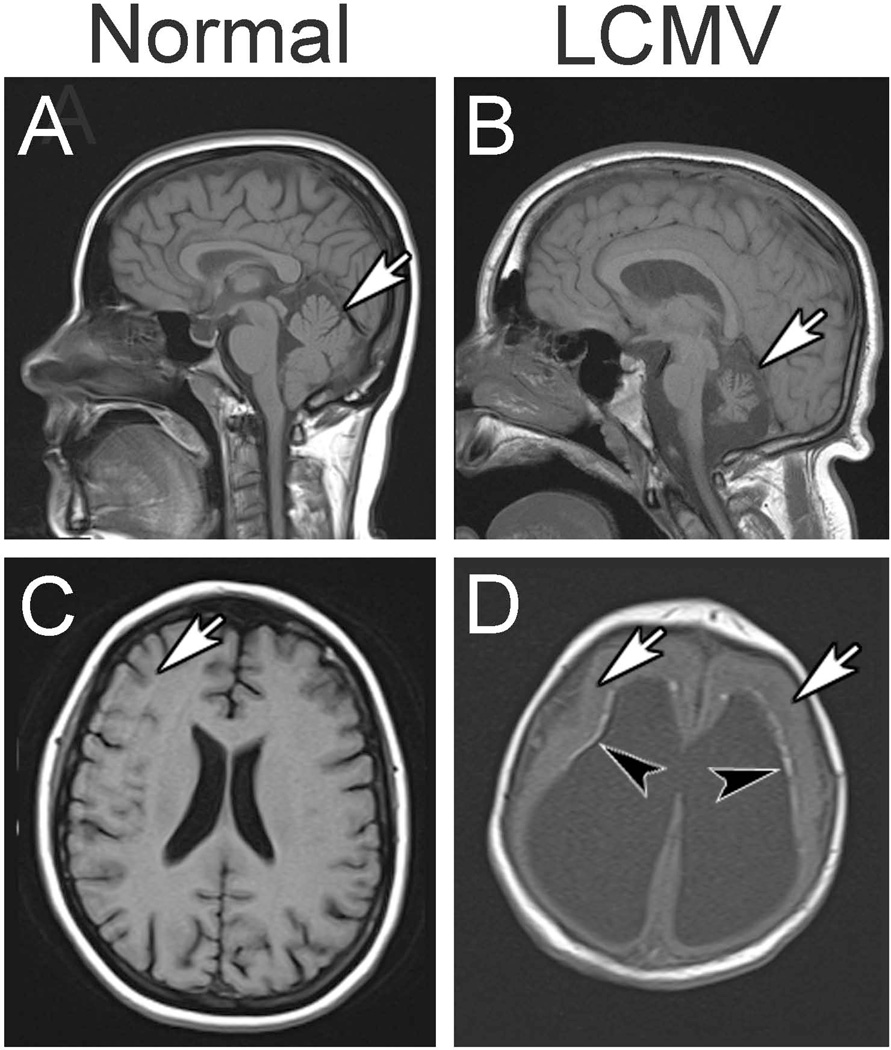
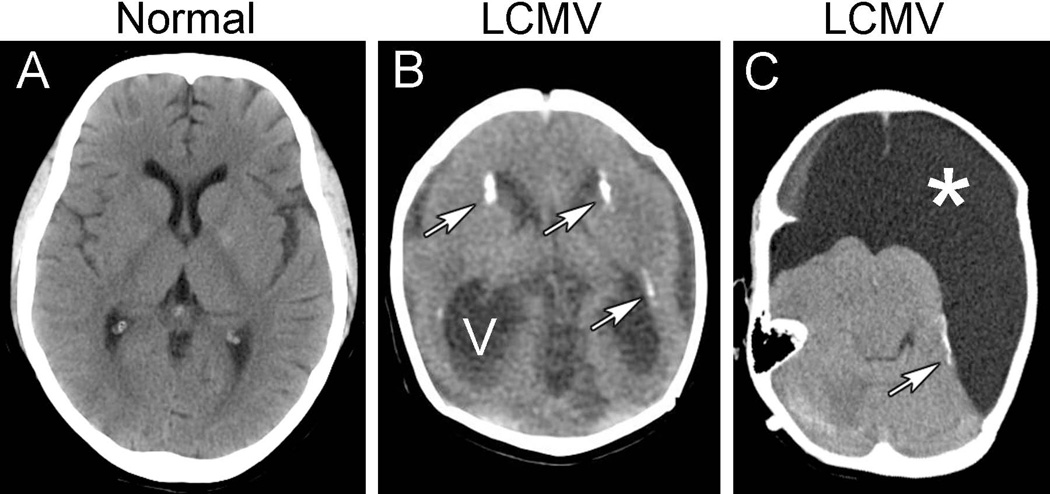
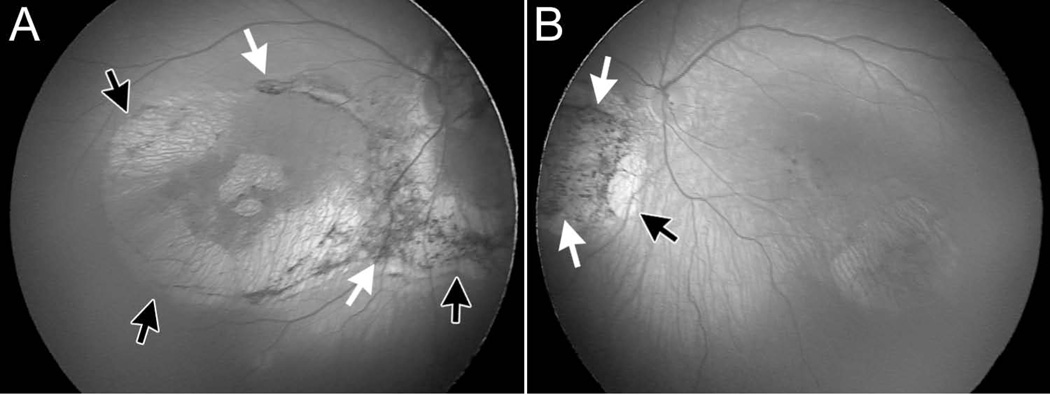
Lymphocytic choriomeningitis virus (LCMV) is an important cause of neurologic disease in humans. Carried and secreted principally by wild mice, LCMV covers a large geographic range and infects great numbers of people. Humans acquire LCMV disease when they come into contact with the secretions of infected mice. Because it has a strong neurotropism, the clinical signs and symptoms of LCMV infection are mostly neurologic. When the virus is acquired postnatally by children or adults, the clinical manifestations are usually those of aseptic meningitis. Most people who acquire LCMV infection during childhood or adulthood are moderately symptomatic for several weeks, but have a full recovery. A much more severe disease ensues when the infection occurs prenatally. LCMV can infect the fetal brain and retina, where it leads to substantial injury and permanent dysfunction. The possibility of LCMV infection should be considered in all babies with evidence of congenital infection, especially those with prominent neurologic signs, such as microencephaly, periventricular calcifications, and hydrocephalus.
Copyright © 2012 Elsevier Inc. All rights reserved.
Figures
References
-
- Buchmeier MJ, Zajac AJ. Lymphocytic choriomeningitis virus. In: Ahmed R, Chen I, editors. Persistent Viral Infections. New York: Wiley; 1999. pp. 575–605.
-
- Bonthius DJ, Barton LL, Klein de Licona H, Bonthius NE, Karacay B. Arenaviruses. In: Barton LL, Friedman NR, editors. The Neurological Manifestations of Pediatric Infectious Diseases and Immunodeficiency Syndromes. Totown, NJ: Humana Press; 2008. pp. 135–150.
-
- Biggar R, Woodall J, Walter P, Haughie G. Lymphocytic choriomeningitis outbreak associated with pet hamsters: fifty seven cases from New York state. JAMA. 1975;232:494. - PubMed
-
- Lehmann-Grube F. Portraits of viruses: arenaviruses. Intervirology. 1984;22:121–145. - PubMed
-
- Fischer SA, Graham MB, Kuehnert M, Kotton CN, Srinivasan A, Marty FM, et al. Transmission of lymphocytic choriomeningitis virus by organ transplantation. New Engl J Med. 2006;354:2235–2249. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
