

Mild hypothermia decreases arrhythmia susceptibility in a canine model of global myocardial ischemia*
- PMID: 22890250
- PMCID: PMC3652239
- DOI: 10.1097/CCM.0b013e31825fd39d
Mild hypothermia decreases arrhythmia susceptibility in a canine model of global myocardial ischemia*
Abstract
Objectives: Although the majority of sudden cardiac arrests occur in patients with ischemic heart disease, the effect of therapeutic hypothermia on arrhythmia susceptibility during acute global ischemia is not well understood. While both ischemia and severe hypothermia are arrhythmogenic, patients undergoing therapeutic hypothermia do not have an increase in arrhythmias, despite the fact that most sudden cardiac arrest occur in the setting of ischemia. We hypothesized that mild hypothermia induced prior to myocardial ischemia and reperfusion will have a beneficial effect on ischemia-related arrhythmia substrates.
Design: We developed a model of global ischemia and reperfusion in the canine wedge preparation to study the transmural electrophysiologic effects of ischemia at different temperatures.
Setting: Animal study.
Subjects: Male mongrel dogs.
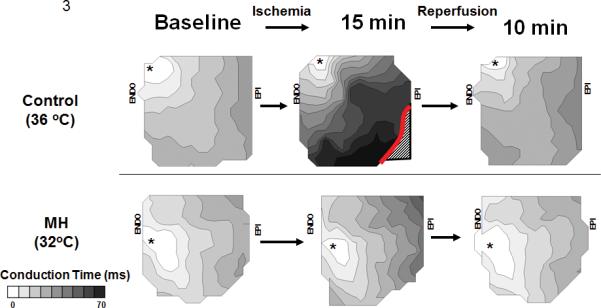
Interventions: Canine left ventricle wedge preparations at 1) control (36°C) or 2) mild hypothermia, to simulate temperatures used in therapeutic hypothermia (32°C), were subjected to 15 mins of no-flow ischemia and subsequently reperfused.
Measurements and main results: Optical action potentials were recorded spanning the transmural wall of left ventricle. Action potential duration for epicardial, mid-myocardial, and epicardial cells was measured. Transmural dispersion of repolarization and conduction velocity were measured at baseline, during ischemia, and during reperfusion. No difference was seen at baseline for conduction velocity or dispersion of repolarization between groups. Conduction velocity decreased from 0.46 ± 0.02 m/sec to 0.23 ± 0.07 m/sec, and dispersion of repolarization increased from 30 ± 5 msecs to 57 ± 4 msecs in the control group at 15 mins of ischemia. Mild hypothermia attenuated both the ischemia-induced conduction velocity slowing (decreasing from 0.44 ± 0.02 m/sec to 0.35 ± 0.03 m/sec; p = .019) and the ischemia-induced increase in dispersion of repolarization (25 ± 3 msecs to 37 ± 7 msecs; p = .037). Epicardial conduction block was observed in six of seven preparations of the control group, but no preparations in the mild hypothermia group developed conduction block (0/6).
Conclusions: Mild hypothermia attenuated ischemia-induced increase in dispersion of repolarization, conduction slowing, and block, which are known mechanisms of arrhythmogenesis in ischemia. These data suggest that therapeutic hypothermia may decrease arrhythmogenesis during myocardial ischemia.
Figures





Comment in
-
The anti-arrhythmic potential of therapeutic hypothermia: another good reason for keeping your cool?*.Crit Care Med. 2012 Nov;40(11):3087-8. doi: 10.1097/CCM.0b013e3182632b08. Crit Care Med. 2012. PMID: 23080441 No abstract available.
References
-
- Zipes DP, Wellens HJ. Sudden cardiac death. Circulation. 1998;98:2334–2351. - PubMed
-
- Nolan JP, Neumar RW, Adrie C, et al. Post-cardiac arrest syndrome: epidemiology, pathophysiology, treatment, and prognostication. A Scientific Statement from the International Liaison Committee on Resuscitation; the American Heart Association Emergency Cardiovascular Care Committee; the Council on Cardiovascular Surgery and Anesthesia; the Council on Cardiopulmonary, Perioperative, and Critical Care; the Council on Clinical Cardiology; the Council on Stroke. Resuscitation. 2008;79:350–379. - PubMed
-
- Bernard SA, Gray TW, Buist MD, et al. Treatment of comatose survivors of out-of-hospital cardiac arrest with induced hypothermia. N Engl J Med. 2002;346:557–563. - PubMed
-
- HACA Investigators Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N Engl J Med. 2002;346:5549–56. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
