

Effectiveness of radiation for prevention of mastectomy in older breast cancer patients treated with conservative surgery
- PMID: 22890779
- PMCID: PMC3884811
- DOI: 10.1002/cncr.27457
Effectiveness of radiation for prevention of mastectomy in older breast cancer patients treated with conservative surgery
Abstract
Background: A recent clinical trial concluded that radiation therapy (RT) does not lower the risk of mastectomy and, thus, may be omitted in older women with stage I, estrogen receptor (ER)-positive breast cancer who undergo conservative surgery (CS). However, it is not known whether this finding applies to patients outside of clinical trials. Accordingly, we used the Surveillance, Epidemiology, and End Results-Medicare observational cohort to determine the effect of RT on the risk of mastectomy among older women with stage I, ER-positive breast cancer.
Methods: The authors identified 7403 women ages 70 to 79 years who underwent CS between 1992 and 2002. Claims were used to determine RT status and to identify women who underwent mastectomy subsequent to initial treatment. The Kaplan-Meier method was used to estimate the risk of subsequent mastectomy, and Cox regression analysis was used to determine the effect of RT adjusted for clinical-pathologic covariates.
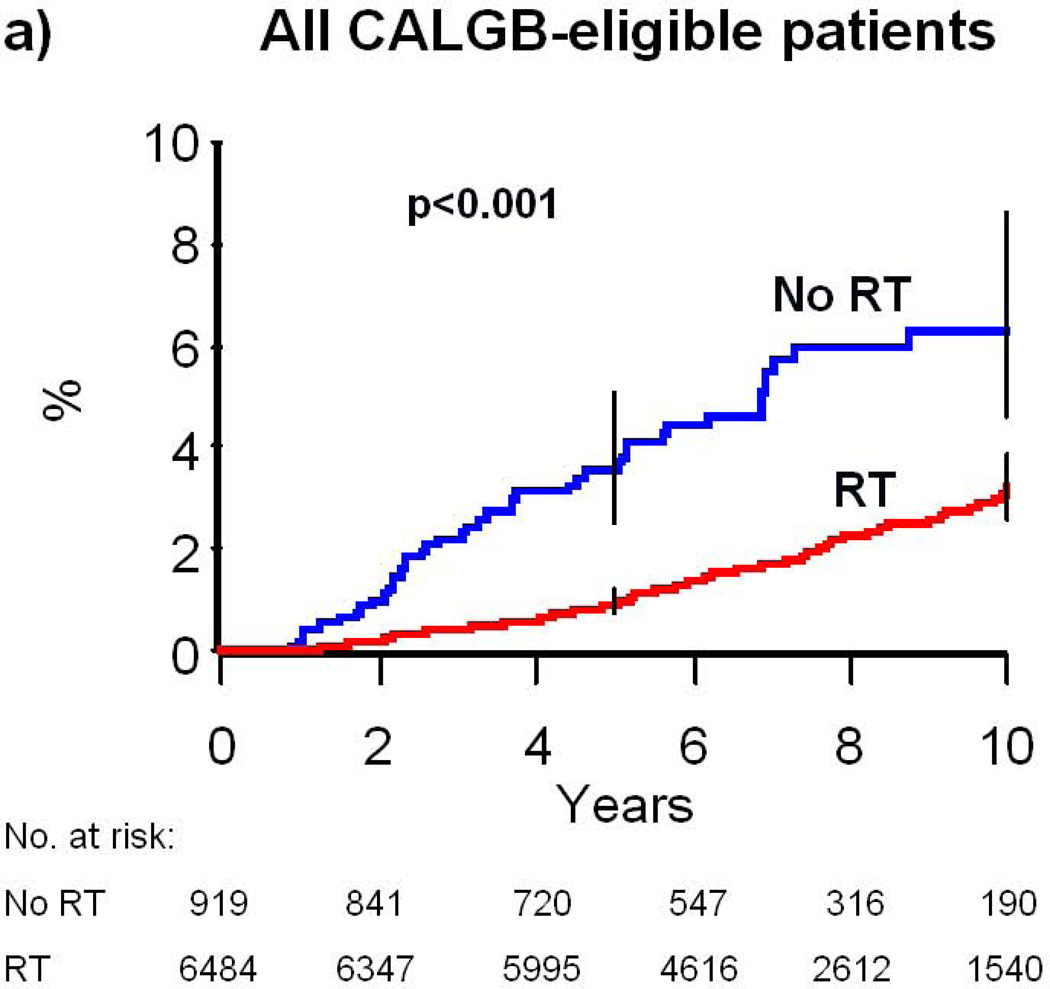
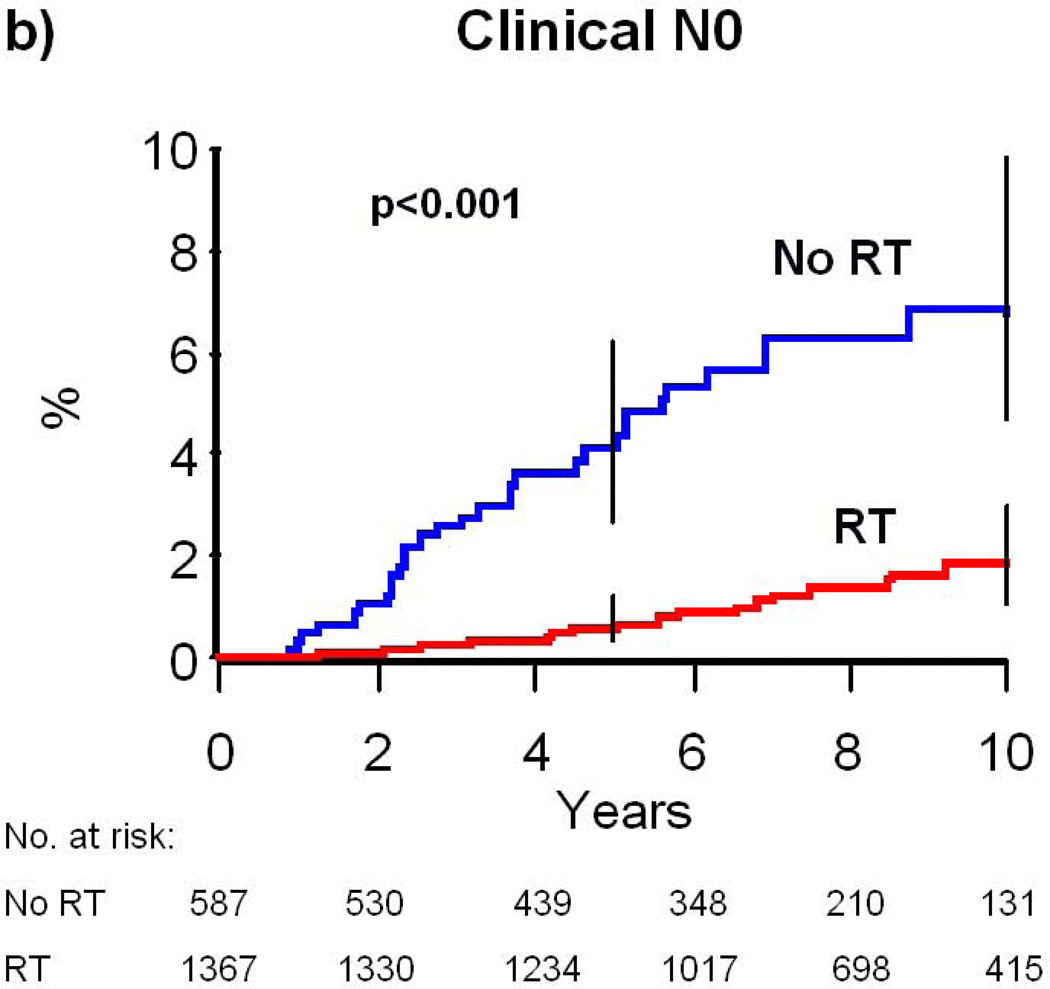
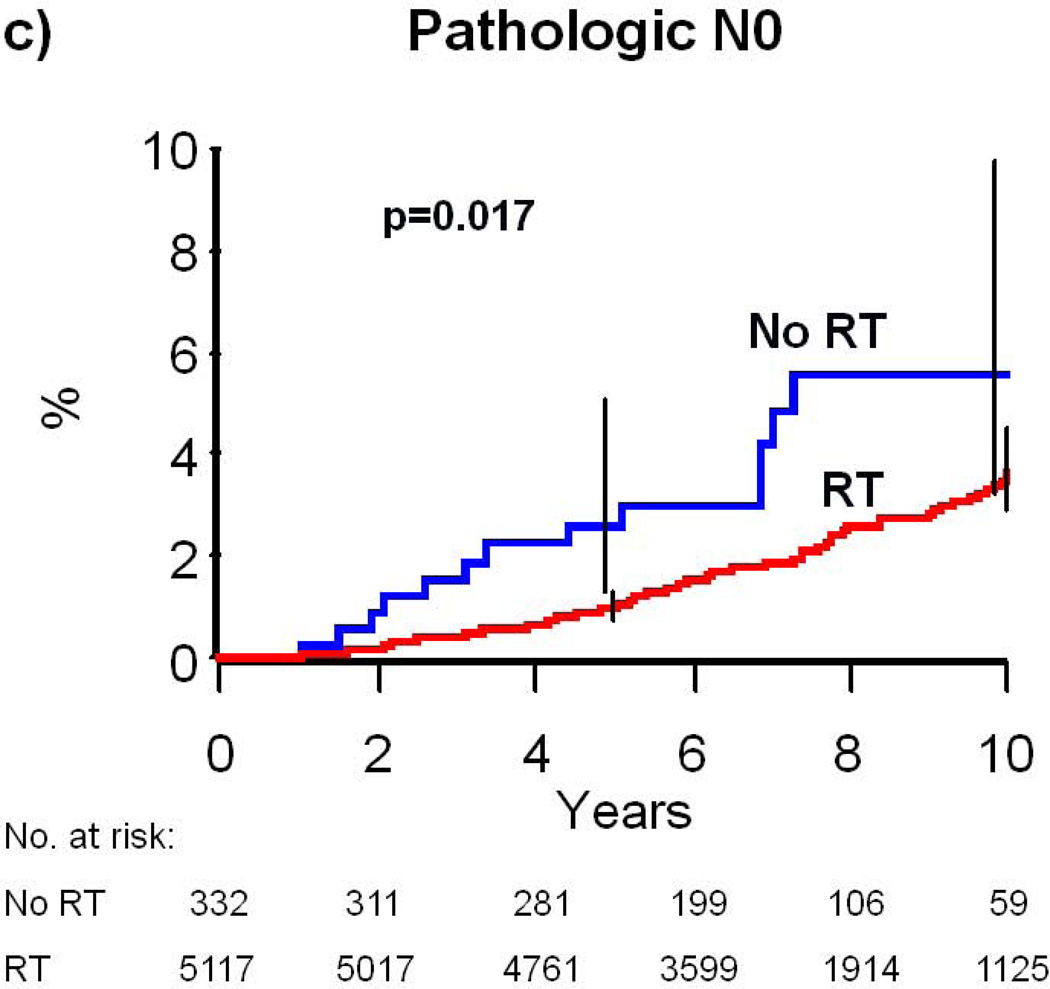
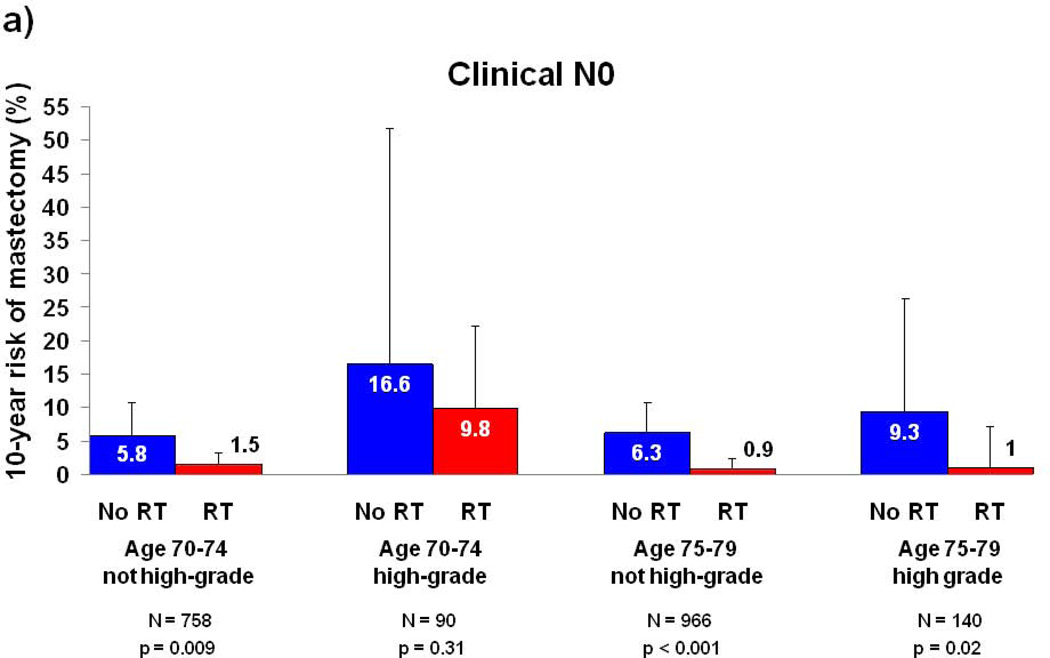
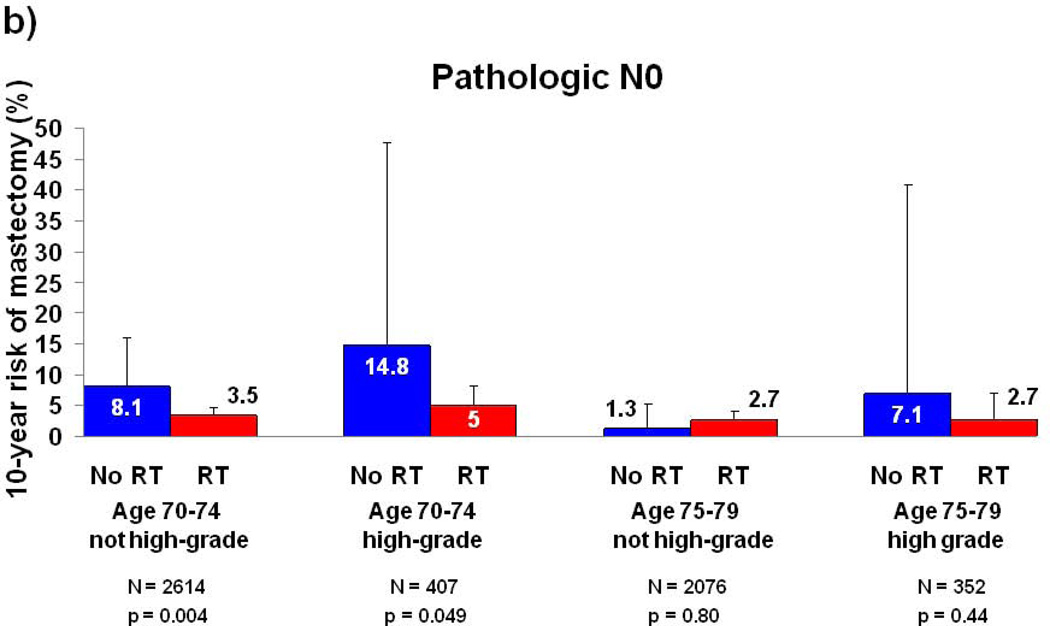
Results: At a median follow-up of 7.3 years, the risk of subsequent mastectomy within 10 years of diagnosis was 3.2% for patients who received RT versus 6.3% for patients who did not receive RT (P < .001). In adjusted analyses, RT was associated with a lower risk of mastectomy (hazard ratio, 0.33; 95% confidence interval, 0.22-0.48; P < .001). RT provided no benefit for patients ages 75 to 79 years without high-grade tumors who had a pathologic lymph node assessment (P = .80); however, for all other subgroups, RT was associated with an absolute reduction in risk of mastectomy that ranged from 4.3% to 9.8% at 10 years.
Conclusions: Outside of a clinical trial, the receipt of RT after CS was associated with a greater likelihood of ultimate breast preservation for most older women with early breast cancer.
Copyright © 2012 American Cancer Society.
Figures
References
-
- Clarke M, Collins R, Darby S, Davies C, Elphinstone P, Evans E, et al. Effects of radiotherapy and of differences in the extent of surgery for early breast cancer on local recurrence and 15-year survival: an overview of the randomised trials. Lancet. 2005;366(9503):2087–2106. - PubMed
-
- Fisher B, Anderson S, Bryant J, Margolese RG, Deutsch M, Fisher ER, et al. Twenty-year follow-up of a randomized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer. N Engl J Med. 2002;347(16):1233–1241. - PubMed
-
- Forrest AP, Stewart HJ, Everington D, Prescott RJ, McArdle CS, Harnett AN, et al. Randomised controlled trial of conservation therapy for breast cancer: 6-year analysis of the Scottish trial. Scottish Cancer Trials Breast Group. Lancet. 1996;348(9029):708–713. - PubMed
-
- Liljegren G, Holmberg L, Bergh J, Lindgren A, Tabar L, Nordgren H, et al. 10-Year results after sector resection with or without postoperative radiotherapy for stage I breast cancer: a randomized trial. J Clin Oncol. 1999;17(8):2326–2333. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
