

Nutrition algorithms for infants with hypoplastic left heart syndrome; birth through the first interstage period
- PMID: 22891735
- PMCID: PMC3618624
- DOI: 10.1111/j.1747-0803.2012.00705.x
Nutrition algorithms for infants with hypoplastic left heart syndrome; birth through the first interstage period
Abstract
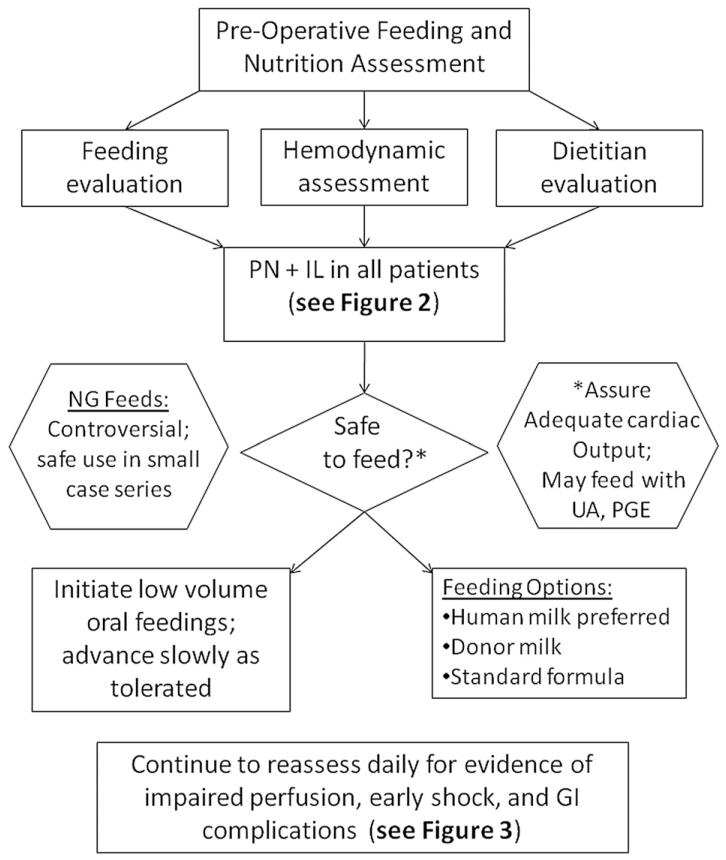
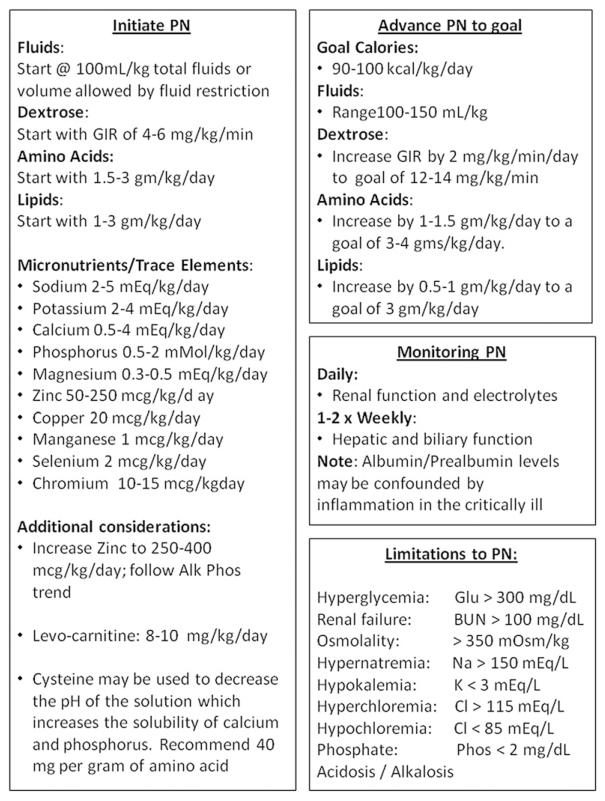
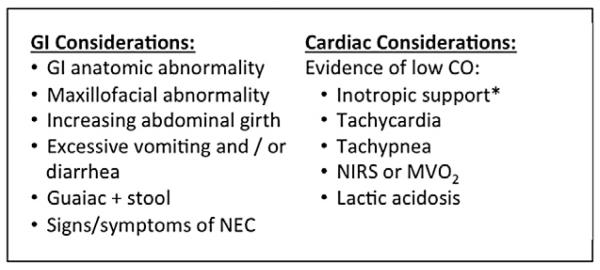
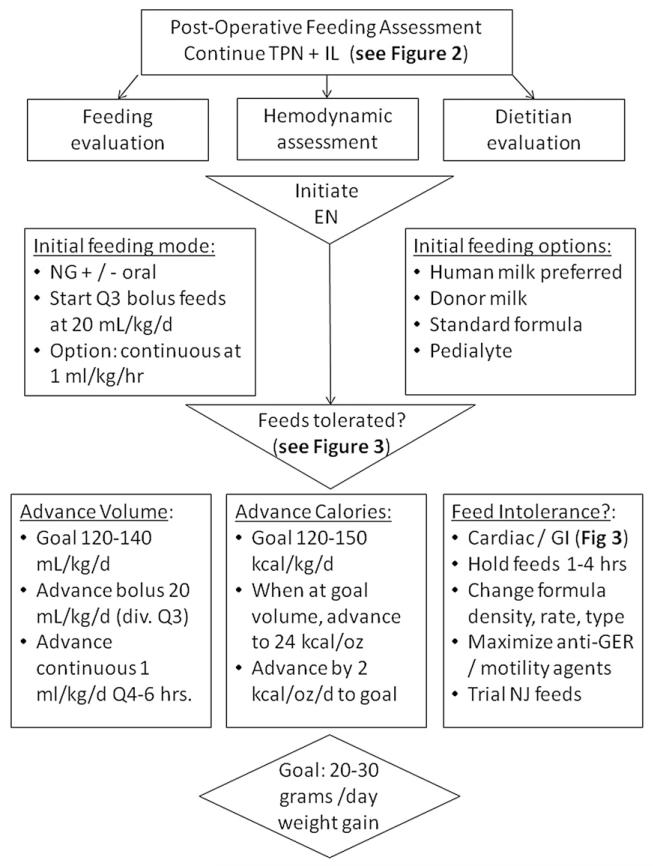
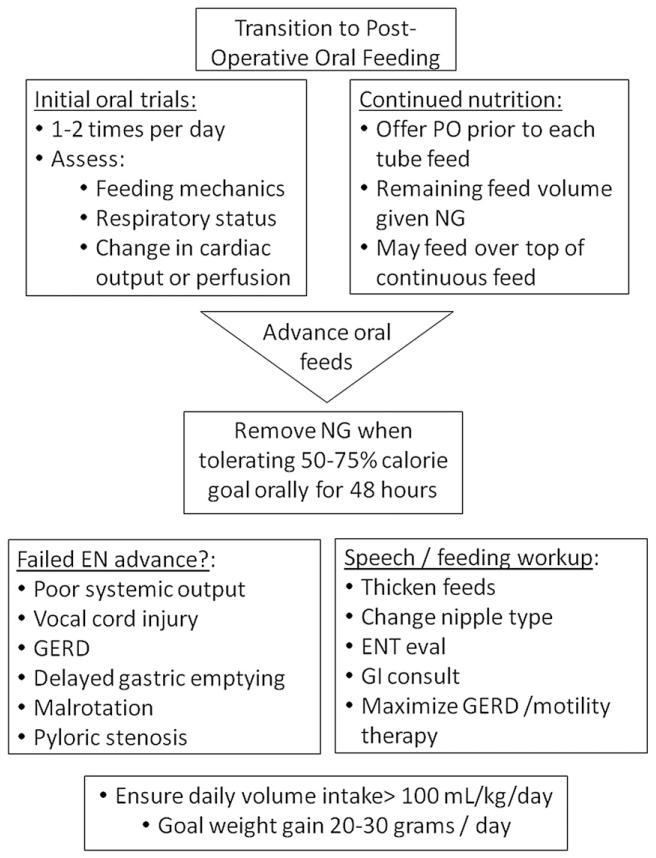
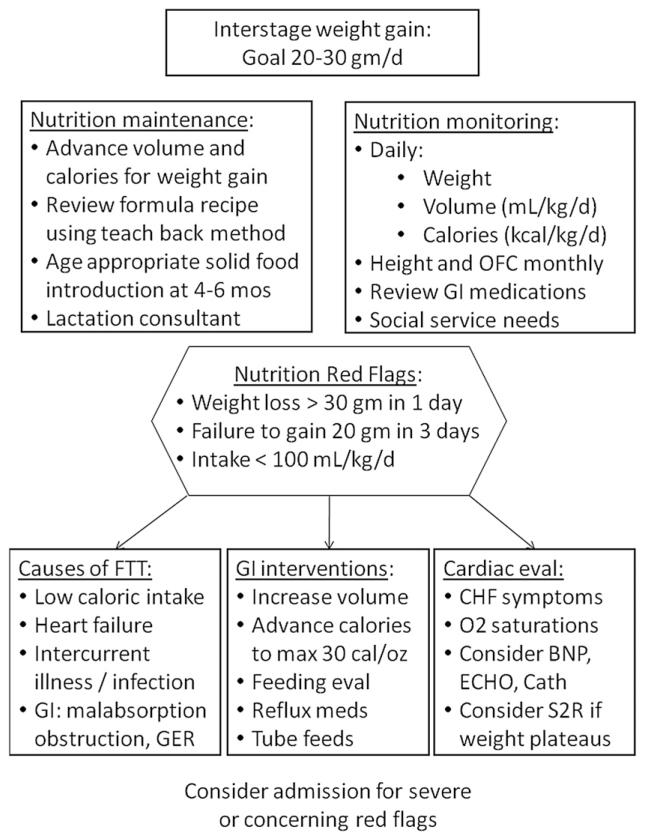
Failure to thrive is common in infants with hypoplastic left heart syndrome and its variants and those with poor growth may be at risk for worse surgical and neurodevelopmental outcomes. The etiology of growth failure in this population is multifactorial and complex, but may be impacted by nutritional intervention. There are no consensus guidelines outlining best practices for nutritional monitoring and intervention in this group of infants. The Feeding Work Group of the National Pediatric Cardiology Quality Improvement Collaborative performed a literature review and assessment of best nutrition practices from centers participating in the collaborative in order to provide nutritional recommendations and levels of evidence for those caring for infants with single ventricle physiology.
© 2012 Wiley Periodicals, Inc.
Figures
References
-
- Krasemann T, Fenge H, Kehl HG, et al. A decade of staged Norwood palliation in hypoplastic left heart syndrome in a midsized cardiosurgical center. Pediatr Cardiol. 2005;26:751–755. - PubMed
-
- Ashburn DA, McCrindle BW, Tchervenkov CI, et al. Outcomes after the Norwood operation in neonates with critical aortic stenosis or aortic valve atresia. J Thorac Cardiovasc Surg. 2003;125:1070–1082. - PubMed
-
- Tweddell JS, Hoffman GM, Mussatto KA, et al. Improved survival of patients undergoing palliation of hypoplastic left heart syndrome: lessons learned from 115 consecutive patients. Circulation. 2002;106:I82–I89. - PubMed
-
- Ohye RG. Multi-institutional studies: lessons learned from the Pediatric Heart Network Single Ventricle Reconstruction Trial. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 2010;13:76–78. - PubMed
-
- Ghanayem NS, Tweddell JS, Hoffman GM, Mussatto K, Jaquiss RD. Optimal timing of the second stage of palliation for hypoplastic left heart syndrome facilitated through home monitoring, and the results of early cavopulmonary anastomosis. Cardiol Young. 2006;16(suppl 1):61–66. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
