

The effects of postprandial glucose and insulin levels on postprandial endothelial function in subjects with normal glucose tolerance
- PMID: 22891922
- PMCID: PMC3471039
- DOI: 10.1186/1475-2840-11-98
The effects of postprandial glucose and insulin levels on postprandial endothelial function in subjects with normal glucose tolerance
Abstract
Background: Previous studies have demonstrated that postprandial hyperglycemia attenuates brachial artery flow-mediated dilation (FMD) in prediabetic patients, in diabetic patients, and even in normal subjects. We have previously reported that postprandial hyperinsulinemia also attenuates FMD. In the present study we evaluated the relationship between different degrees of postprandial attenuation of FMD induced by postprandial hyperglycemia and hyperinsulinemia and differences in ingested carbohydrate content in non-diabetic individuals.
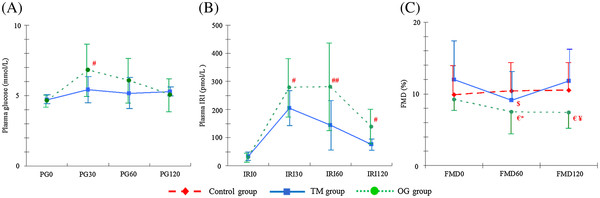
Methods: Thirty-seven healthy subjects with no family history of diabetes were divided into 3 groups: a 75-g oral glucose loading group (OG group) (n = 14), a test meal group (TM group) (n = 12; 400 kcal, carbohydrate content 40.7 g), and a control group (n = 11). The FMD was measured at preload (FMD0) and at 60 minutes (FMD60) and 120 (FMD120) minutes after loading. Plasma glucose (PG) and immunoreactive insulin (IRI) levels were determined at preload (PG0, IRI0) and at 30 (PG30, IRI30), 60 (PG60, IRI60), and 120 (PG120, IRI120) minutes after loading.
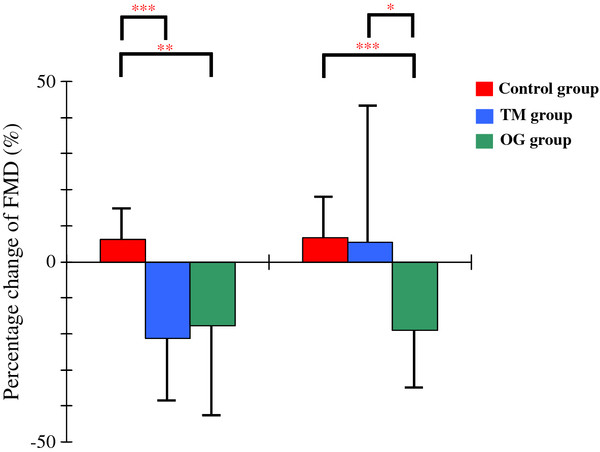
Result: Percentage decreases from FMD0 to FMD60 were significantly greater in the TM group (-21.19% ± 17.90%; P < 0.001) and the OG group (-17.59% ± 26.64%) than in the control group (6.46% ± 9.17%; P < 0.01), whereas no significant difference was observed between the TM and OG groups. In contrast, the percentage decrease from FMD0 to FMD120 was significantly greater in the OG group (-18.91% ± 16.58%) than in the control group (6.78% ± 11.43%; P < 0.001) or the TM group (5.22% ± 37.22%; P < 0.05), but no significant difference was observed between the control and TM groups. The FMD60 was significantly correlated with HOMA-IR (r = -0.389; P < 0.05). In contrast, FMD120 was significantly correlated with IRI60 (r = -0.462; P < 0.05) and the AUC of IRI (r = -0.468; P < 0.05). Furthermore, the percentage change from FMD0 to FMD120 was significantly correlated with the CV of PG (r = 0.404; P < 0.05), IRI60 (r = 0.401; p < 0.05) and the AUC of IRI (r = 0.427; P < 0.05). No significant correlation was observed between any other FMDs and glucose metabolic variables.
Conclusion: Differences in the attenuation of postprandial FMD induced by different postprandial insulin levels may occur a long time postprandially but not shortly after a meal.
Figures
Similar articles
-
Effects of 6-month eicosapentaenoic acid treatment on postprandial hyperglycemia, hyperlipidemia, insulin secretion ability, and concomitant endothelial dysfunction among newly-diagnosed impaired glucose metabolism patients with coronary artery disease. An open label, single blinded, prospective randomized controlled trial.Cardiovasc Diabetol. 2016 Aug 26;15(1):121. doi: 10.1186/s12933-016-0437-y. Cardiovasc Diabetol. 2016. PMID: 27565734 Free PMC article.
-
Aerobic or resistance exercise performed the previous day does not attenuate postprandial hyperglycemia-induced endothelial dysfunction in overweight/obese adults.Eur J Appl Physiol. 2019 Aug;119(8):1855-1863. doi: 10.1007/s00421-019-04174-x. Epub 2019 Jun 11. Eur J Appl Physiol. 2019. PMID: 31187279 Clinical Trial.
-
Postprandial hyperglycemia impairs vascular endothelial function in healthy men by inducing lipid peroxidation and increasing asymmetric dimethylarginine:arginine.J Nutr. 2011 Nov;141(11):1961-8. doi: 10.3945/jn.111.144592. Epub 2011 Sep 21. J Nutr. 2011. PMID: 21940510 Clinical Trial.
-
Effect of glycemic state on postprandial hyperlipidemia and hyperinsulinemia in patients with coronary artery disease.Heart Vessels. 2016 Sep;31(9):1446-55. doi: 10.1007/s00380-015-0757-y. Epub 2015 Oct 6. Heart Vessels. 2016. PMID: 26439243 Free PMC article.
-
Postprandial endothelial dysfunction: role of glucose, lipids and insulin.Diabetes Metab. 2006 Sep;32 Spec No2:2S28-33. doi: 10.1016/s1262-3636(06)70482-7. Diabetes Metab. 2006. PMID: 17375404 Review.
Cited by
-
Dietary macronutrients do not differently affect postprandial vascular endothelial function in apparently healthy overweight and slightly obese men.Eur J Nutr. 2021 Apr;60(3):1443-1451. doi: 10.1007/s00394-020-02340-y. Epub 2020 Jul 29. Eur J Nutr. 2021. PMID: 32728881 Free PMC article. Clinical Trial.
-
A single consumption of curry improved postprandial endothelial function in healthy male subjects: a randomized, controlled crossover trial.Nutr J. 2014 Jun 28;13:67. doi: 10.1186/1475-2891-13-67. Nutr J. 2014. PMID: 24972677 Free PMC article. Clinical Trial.
-
Endothelial function following interval exercise plus low-calorie diet treatment in obese females.Physiol Rep. 2019 Sep;7(18):e14239. doi: 10.14814/phy2.14239. Physiol Rep. 2019. PMID: 31552710 Free PMC article. Clinical Trial.
-
The Postprandial Appearance of Features of Cardiometabolic Risk: Acute Induction and Prevention by Nutrients and Other Dietary Substances.Nutrients. 2019 Aug 21;11(9):1963. doi: 10.3390/nu11091963. Nutrients. 2019. PMID: 31438565 Free PMC article. Review.
-
Flow Mediated Dilatation Is Reduced with the Progressive Stages of Glomerular Filtration Rate and Albuminuria in Type 2 Diabetic Patients without Coronary Heart Disease.J Diabetes Res. 2015;2015:728127. doi: 10.1155/2015/728127. Epub 2015 Apr 29. J Diabetes Res. 2015. PMID: 26064988 Free PMC article.
References
-
- The DECODE study group on behalf of the European Diabetes Epidemiology Group. Glucose tolerance and mortality: comparison of WHO and American Diabetic Association diagnostic criteria. Lancet. 1999;354:617–621. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
