

Comparison of rectal and aural core body temperature thermometry in hyperthermic, exercising individuals: a meta-analysis
- PMID: 22892415
- PMCID: PMC3392164
- DOI: 10.4085/1062-6050-47.3.09
Comparison of rectal and aural core body temperature thermometry in hyperthermic, exercising individuals: a meta-analysis
Erratum in
- J Athl Train. 2014 Jan-Feb;49(1):138
Abstract
Objective: To compare mean differences in core body temperature (T(core)) as assessed via rectal thermometry (T(re)) and aural thermometry (T(au)) in hyperthermic exercising individuals.
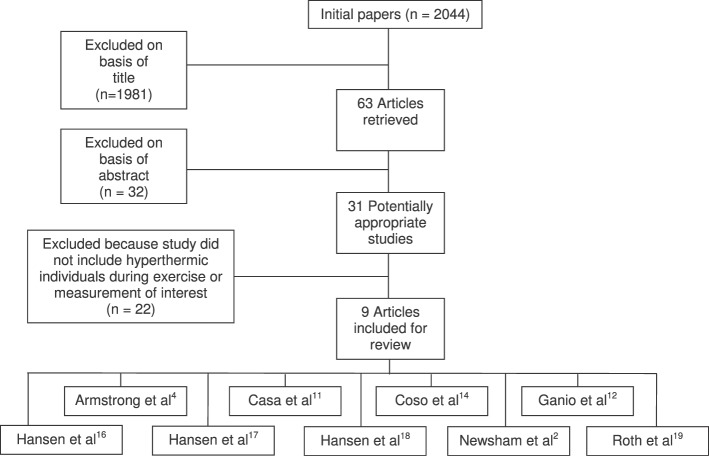
Data sources: PubMed, Ovid MEDLINE, SPORTDiscus, CINAHL, and Cochrane Library in English from the earliest entry points to August 2009 using the search terms aural, core body temperature, core temperature, exercise, rectal, temperature, thermistor, thermometer, thermometry, and tympanic. Study Selection: Original research articles that met these criteria were included: (1) concurrent measurement of T(re) and T(au) in participants during exercise, (2) minimum mean temperature that reached 38°C by at least 1 technique during or after exercise, and (3) report of means, standard deviations, and sample sizes.
Data extraction: Nine articles were included, and 3 independent reviewers scored these articles using the Physiotherapy Evidence Database (PEDro) scale (mean = 5.1 ± 0.4). Data were divided into time periods pre-exercise, during exercise (30 to 180 minutes), and postexercise, as well as T(re) ranges <37.99°C, 38.00°C to 38.99°C, and >39.00°C. Means and standard deviations for both measurement techniques were provided at all time intervals reported. Meta-analysis was performed to determine pooled and weighted mean differences between T(re) and T(au).
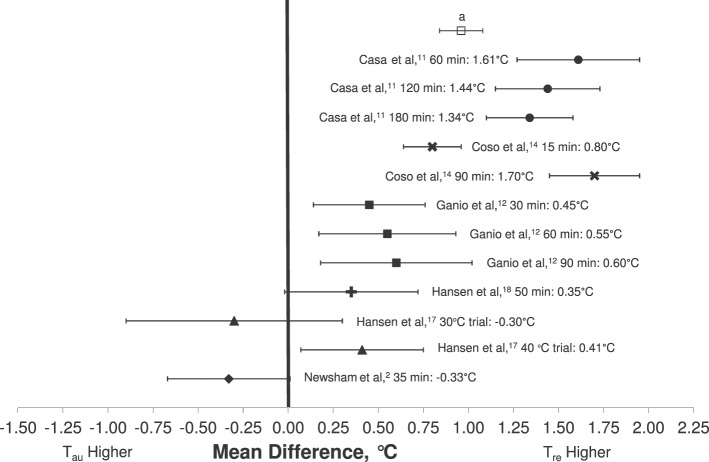
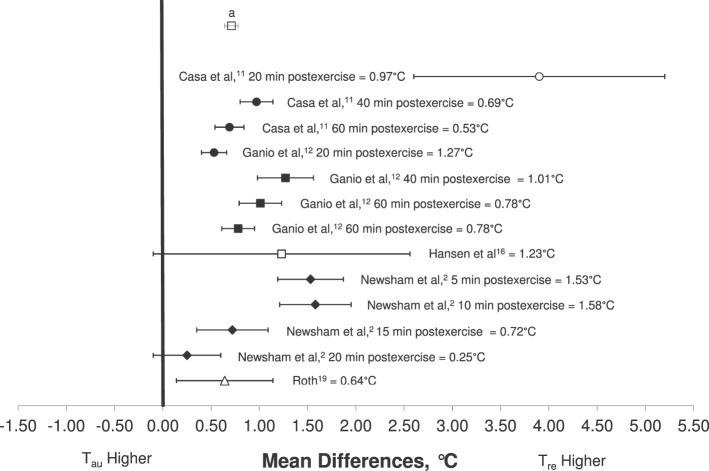
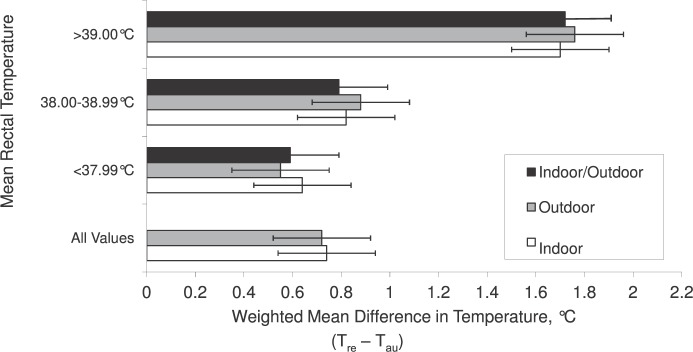
Data synthesis: The T(re) was conclusively higher than the T(au) pre-exercise (mean difference [MD] = 0.27°C, 95% confidence interval [CI] = 0.15°C, 0.39°C), during exercise (MD = 0.96°C, 95% CI = 0.84°C, 1.08°C), and postexercise (MD = 0.71°C, 95% CI = 0.65°C, 0.78°C). As T(re) measures increased, the magnitude of difference between the techniques also increased with an MD of 0.59°C (95% CI = 0.53°C, 0.65°C) when T(re) was <38°C; 0.79°C (95% CI = 0.72°C, 0.86°C) when T(re) was between 38.0°C and 38.99°C; and 1.72°C (95% CI = 1.54°, 1.91°C) when T(re) was >39.0°C.
Conclusions: The T(re) was consistently greater than T(au) when T(core) was measured in hyperthermic individuals before, during, and postexercise. As T(core) increased, T(au) appeared to underestimate T(core) as determined by T(re). Clinicians should be aware of this critical difference in temperature magnitude between these measurement techniques when assessing T(core) in hyperthermic individuals during or postexercise.
Figures
Similar articles
-
Validity and reliability of devices that assess body temperature during indoor exercise in the heat.J Athl Train. 2009 Mar-Apr;44(2):124-35. doi: 10.4085/1062-6050-44.2.124. J Athl Train. 2009. PMID: 19295956 Free PMC article.
-
Optimizing Cold-Water Immersion for Exercise-Induced Hyperthermia: An Evidence-Based Paper.J Athl Train. 2016 Jun 2;51(6):500-1. doi: 10.4085/1062-6050-51.9.04. Epub 2016 Jul 21. J Athl Train. 2016. PMID: 27441949 Free PMC article. Review.
-
Validity of devices that assess body temperature during outdoor exercise in the heat.J Athl Train. 2007 Jul-Sep;42(3):333-42. J Athl Train. 2007. PMID: 18059987 Free PMC article.
-
Temporal artery thermometry in children younger than 5 years: a comparison with rectal thermometry.Pediatr Emerg Care. 2014 Dec;30(12):867-70. doi: 10.1097/PEC.0000000000000289. Pediatr Emerg Care. 2014. PMID: 25407036
-
Temporal Artery Thermometry in Pediatric Patients: Systematic Review and Meta-Analysis.J Pediatr Nurs. 2019 May-Jun;46:89-99. doi: 10.1016/j.pedn.2019.03.004. Epub 2019 Mar 10. J Pediatr Nurs. 2019. PMID: 30865876
Cited by
-
Exertional Heat-Stroke Management Practices and Intentions Among Secondary School Football Athletic Trainers.J Athl Train. 2020 Oct 1;55(10):1081-1088. doi: 10.4085/1062-6050-474-19. J Athl Train. 2020. PMID: 32966554 Free PMC article.
-
Evaluation of the physiological changes in prehospital health-care providers influenced by environmental factors in the summer of 2020 during the COVID-19 pandemic.Acute Med Surg. 2021 Oct 28;8(1):e699. doi: 10.1002/ams2.699. eCollection 2021 Jan-Dec. Acute Med Surg. 2021. PMID: 34745638 Free PMC article.
-
National Athletic Trainers' Association Position Statement: Exertional Heat Illnesses.J Athl Train. 2015 Sep;50(9):986-1000. doi: 10.4085/1062-6050-50.9.07. J Athl Train. 2015. PMID: 26381473 Free PMC article.
-
The roles of ACE I/D and ACTN3 R577X gene variants in heat acclimation.Heliyon. 2024 Jun 15;10(12):e33172. doi: 10.1016/j.heliyon.2024.e33172. eCollection 2024 Jun 30. Heliyon. 2024. PMID: 38984309 Free PMC article.
-
Classic and exertional heatstroke.Nat Rev Dis Primers. 2022 Feb 3;8(1):8. doi: 10.1038/s41572-021-00334-6. Nat Rev Dis Primers. 2022. PMID: 35115565 Review.
References
-
- Mueller FO, Colgate B. Annual survey of football injury research, 1931–2009. http://www.unc.edu/depts/nccsi/2009AnnualFootball.pdf. Accessed December 16, 2011.
-
- Newsham KR, Saunders JE, Nordin ES. Comparison of rectal and tympanic thermometry during exercise. South Med J. 2002;95(8):804–810. - PubMed
-
- Pandolf KB, Takeda N, Singal PK. Adaptation Biology and Medicine: Volume 2. Molecular Basis. New Delhi, India: Narosa Publishing House; 1999.
-
- Armstrong L, Maresh C, Crago A, Adams R, Roberts W. Interpretation of aural temperatures during exercise, hyperthermia, and cooling therapy. Med Exerc Nutr Health. 1994;3(1):9–16.
-
- Casa DJ, Armstrong LE, Ganio MS, Yeargin SW. Exertional heat stroke in competitive athletes. Curr Sports Med Rep. 2005;4(6):309–317. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
