

Adult low-grade glioma: 19-year experience at a single institution
- PMID: 22892428
- PMCID: PMC4361933
- DOI: 10.1097/COC.0b013e31825d580a
Adult low-grade glioma: 19-year experience at a single institution
Abstract
Objectives: To determine prognostic factors and optimal timing of postoperative radiation therapy (RT) in adult low-grade gliomas.
Methods: Records from 554 adults diagnosed with nonpilocytic low-grade gliomas at Mayo Clinic between 1992 and 2011 were retrospectively reviewed.
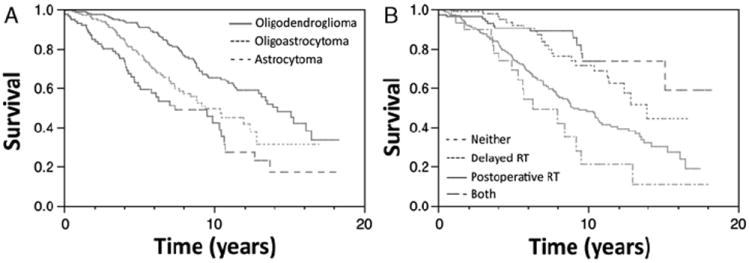
Results: Median follow-up was 5.2 years. Histology revealed astrocytoma in 22%, oligoastrocytoma in 34%, and oligodendroglioma in 45%. Initial surgery achieved gross total resection in 31%, radical subtotal resection in 10%, subtotal resection (STR) in 21%, and biopsy only in 39%. Median overall survival (OS) and progression-free survival (PFS) were 11.4 and 4.1 years, respectively. On multivariate analysis, factors associated with lower OS included astrocytomas and use of postoperative RT. Adverse prognostic factors for PFS on multivariate analysis included tumor size, astrocytomas, STR/biopsy only and not receiving RT. Patients undergoing gross total resection/radical subtotal resection had the best OS and PFS. Comparing survival with the log-rank test demonstrated no association between RT and PFS (P=0.24), but RT was associated with lower OS (P<0.0001). In patients undergoing STR/biopsy only, RT was associated with improved PFS (P<0.0001) but lower OS (P=0.03). Postoperative RT was associated with adverse prognostic factors including age > 40 years, deep tumors, size≥5 cm, astrocytomas and STR/biopsy only. Patients delaying RT until recurrence experienced 10-year OS (71%) similar to patients never needing RT (74%; P=0.34).
Conclusions: This study supports the association between aggressive surgical resection and better OS and PFS, and between postoperative RT and improved PFS in patients receiving STR/biopsy only. In addition, our findings suggest that delaying RT until progression is safe in patients who are eligible.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures



References
-
- Janny P, Cure H, Mohr M, et al. Low grade supratentorial astrocytomas. Management and prognostic factors. Cancer. 1994;73:1937–1945. - PubMed
-
- Leighton C, Fisher B, Bauman G, et al. Supratentorial low-grade glioma in adults: an analysis of prognostic factors and timing of radiation. J Clin Oncol. 1997;15:1294–1301. - PubMed
-
- Shaw EG, Daumas-Duport C, Scheithauer BW, et al. Radiation therapy in the management of low-grade supratentorial astrocytomas. J Neurosurg. 1989;70:853–861. - PubMed
-
- Karim AB, Afra D, Cornu P, et al. Randomized trial on the efficacy of radiotherapy for cerebral low-grade glioma in the adult: European Organization for Research and Treatment of Cancer Study 22845 with the Medical Research Council study BRO4: an interim analysis. Int J Radiat Oncol Biol Phys. 2002;52:316–324. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
