

Population versus customized fetal growth norms and adverse outcomes in an intrapartum cohort
- PMID: 22893556
- PMCID: PMC3622136
- DOI: 10.1055/s-0032-1324708
Population versus customized fetal growth norms and adverse outcomes in an intrapartum cohort
Abstract
Objective: To compare population versus customized fetal growth norms in identifying neonates at risk for adverse outcomes (APO) associated with small for gestational age (SGA).
Study design: Secondary analysis of an intrapartum fetal pulse oximetry trial in nulliparous women at term. Birth weight percentiles were calculated using ethnicity- and gender-specific population norms and customized norms (Gardosi).
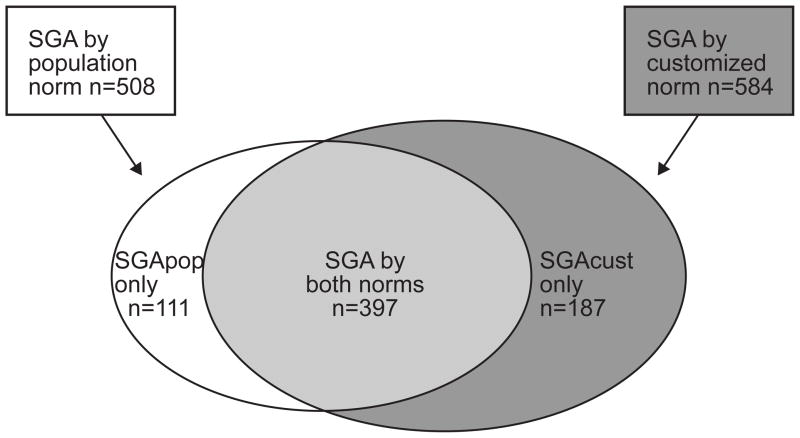
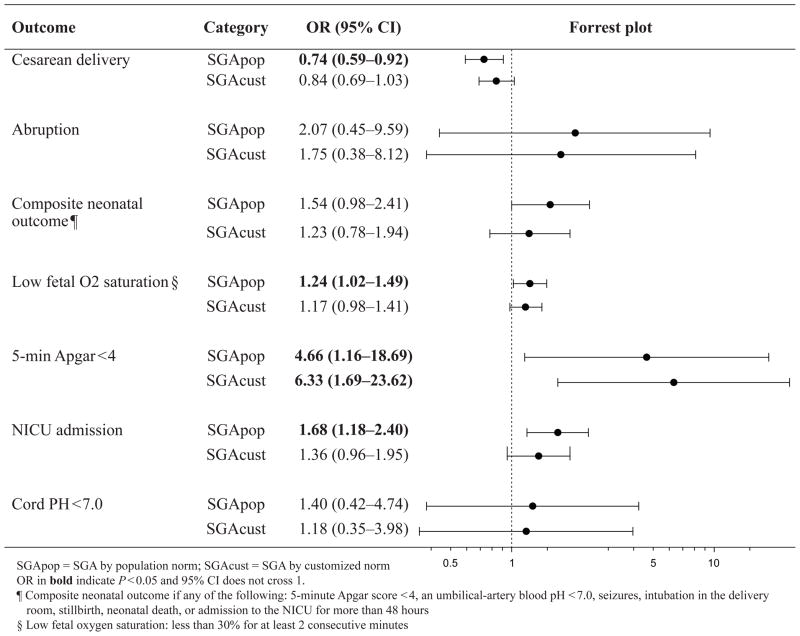
Results: Of the studied neonates, 508 (9.9%) and 584 (11.3%) were SGA by population (SGApop) and customized (SGAcust) norms, respectively. SGApop infants were significantly associated with a composite adverse neonatal outcome, neonatal intensive care admission, low fetal oxygen saturation, and reduced risk of cesarean delivery; both SGApop and SGAcust infants were associated with a 5-minute Apgar score < 4. The ability of customized and population birth weight percentiles in predicting APO was poor (12 of 14 APOs had area under the curve of <0.6).
Conclusion: In this intrapartum cohort, neither customized nor normalized population norms adequately identified neonates at risk of APO related to SGA.
Thieme Medical Publishers 333 Seventh Avenue, New York, NY 10001, USA.
Conflict of interest statement
Disclosure: None of the authors have a conflict of interest
Figures
References
-
- McIntire DD, Bloom SL, Casey BM, Leveno KJ. Birth weight in relation to morbidity and mortality among newborn infants. N Engl J Med. 1999;340:1234–8. - PubMed
-
- Schoendorf KC, Hogue CJ, Kleinman JC, Rowley D. Mortality among infants of black as compared with white college educated parents. N Engl J Med. 1992;326:1522–6. - PubMed
-
- Kajantie E, Osmond C, Barker DJ, Forsen T, Phillips DI, Eriksson JG. Size at birth as a predictor of mortality in adulthood: a follow-up of 350 000 person-years. Int J epidemiol. 2005;34:655–63. - PubMed
-
- Barker DJ, Osmond C, Forsen TJ, Kajantie E, Eriksson JG. Trajectories of growth among children who have coronary events as adults. N Engl J Med. 2005;353:1802–9. - PubMed
-
- Ozanne SE, Fernandez-Twinn D, Hales CN. Fetal growth and adult dieseases. Semin Perinatol. 2004;28:81–87. - PubMed
Publication types
MeSH terms
Grants and funding
- HD36801/HD/NICHD NIH HHS/United States
- U10 HD040500/HD/NICHD NIH HHS/United States
- UG1 HD027869/HD/NICHD NIH HHS/United States
- U10 HD040544/HD/NICHD NIH HHS/United States
- U10 HD034136/HD/NICHD NIH HHS/United States
- U10 HD040485/HD/NICHD NIH HHS/United States
- HD40485/HD/NICHD NIH HHS/United States
- HD40560/HD/NICHD NIH HHS/United States
- U10 HD040560/HD/NICHD NIH HHS/United States
- U10 HD040512/HD/NICHD NIH HHS/United States
- U01 HD036801/HD/NICHD NIH HHS/United States
- UG1 HD034116/HD/NICHD NIH HHS/United States
- HD27869/HD/NICHD NIH HHS/United States
- HD34136/HD/NICHD NIH HHS/United States
- UG1 HD040560/HD/NICHD NIH HHS/United States
- HD27860/HD/NICHD NIH HHS/United States
- UG1 HD027915/HD/NICHD NIH HHS/United States
- HD40512/HD/NICHD NIH HHS/United States
- UG1 HD040544/HD/NICHD NIH HHS/United States
- UG1 HD034208/HD/NICHD NIH HHS/United States
- UG1 HD040512/HD/NICHD NIH HHS/United States
- HD40545/HD/NICHD NIH HHS/United States
- U10 HD034116/HD/NICHD NIH HHS/United States
- HD21410/HD/NICHD NIH HHS/United States
- U10 HD027869/HD/NICHD NIH HHS/United States
- U10 HD027917/HD/NICHD NIH HHS/United States
- HD34116/HD/NICHD NIH HHS/United States
- U10 HD027915/HD/NICHD NIH HHS/United States
- UG1 HD040545/HD/NICHD NIH HHS/United States
- UG1 HD040485/HD/NICHD NIH HHS/United States
- U10 HD027860/HD/NICHD NIH HHS/United States
- HD40500/HD/NICHD NIH HHS/United States
- U10 HD034208/HD/NICHD NIH HHS/United States
- U10 HD053097/HD/NICHD NIH HHS/United States
- HD34208/HD/NICHD NIH HHS/United States
- HD27915/HD/NICHD NIH HHS/United States
- UG1 HD040500/HD/NICHD NIH HHS/United States
- HD27917/HD/NICHD NIH HHS/United States
- U10 HD021410/HD/NICHD NIH HHS/United States
- U10 HD036801/HD/NICHD NIH HHS/United States
- U24 HD036801/HD/NICHD NIH HHS/United States
- U10 HD040545/HD/NICHD NIH HHS/United States
- HD40544/HD/NICHD NIH HHS/United States
