

Changes in incidence and antifungal drug resistance in candidemia: results from population-based laboratory surveillance in Atlanta and Baltimore, 2008-2011
- PMID: 22893576
- PMCID: PMC4698872
- DOI: 10.1093/cid/cis697
Changes in incidence and antifungal drug resistance in candidemia: results from population-based laboratory surveillance in Atlanta and Baltimore, 2008-2011
Abstract
Background: Candidemia is common and associated with high morbidity and mortality; changes in population-based incidence rates have not been reported.
Methods: We conducted active, population-based surveillance in metropolitan Atlanta, Georgia, and Baltimore City/County, Maryland (combined population 5.2 million), during 2008-2011. We calculated candidemia incidence and antifungal drug resistance compared with prior surveillance (Atlanta, 1992-1993; Baltimore, 1998-2000).
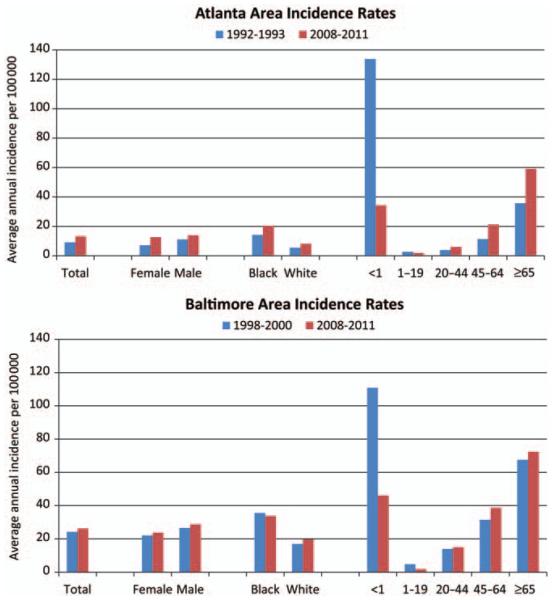
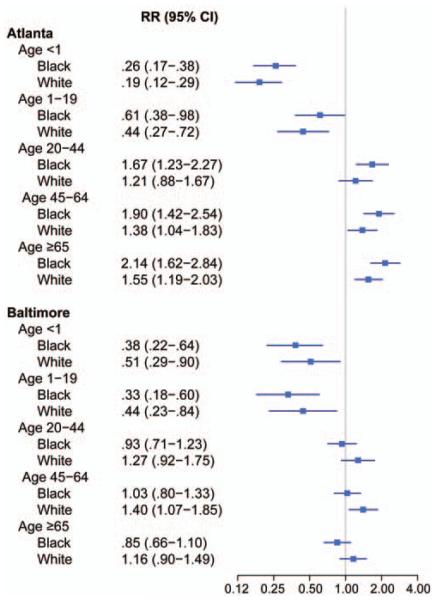
Results: We identified 2675 cases of candidemia with 2329 isolates during 3 years of surveillance. Mean annual crude incidence per 100 000 person-years was 13.3 in Atlanta and 26.2 in Baltimore. Rates were highest among adults aged ≥65 years (Atlanta, 59.1; Baltimore, 72.4) and infants (aged <1 year; Atlanta, 34.3; Baltimore, 46.2). In both locations compared with prior surveillance, adjusted incidence significantly declined for infants of both black and white race (Atlanta: black risk ratio [RR], 0.26 [95% confidence interval {CI}, .17-.38]; white RR: 0.19 [95% CI, .12-.29]; Baltimore: black RR, 0.38 [95% CI, .22-.64]; white RR: 0.51 [95% CI: .29-.90]). Prevalence of fluconazole resistance (7%) was unchanged compared with prior surveillance; 32 (1%) isolates were echinocandin-resistant, and 9 (8 Candida glabrata) were multidrug resistant to both fluconazole and an echinocandin.
Conclusions: We describe marked shifts in candidemia epidemiology over the past 2 decades. Adults aged ≥65 years replaced infants as the highest incidence group; adjusted incidence has declined significantly in infants. Use of antifungal prophylaxis, improvements in infection control, or changes in catheter insertion practices may be contributing to these declines. Further surveillance for antifungal resistance and efforts to determine effective prevention strategies are needed.
Figures
References
-
- Wisplinghoff H, Bischoff T, Tallent SM, Seifert H, Wenzel RP, Edmond MB. Nosocomial bloodstream infections in US hospitals: analysis of 24 179 cases from a prospective nationwide surveillance study. Clin Infect Dis. 2004;39:309–17. - PubMed
-
- Zaoutis TE, Argon J, Chu J, Berlin JA, Walsh TJ, Feudtner C. The epidemiology and attributable outcomes of candidemia in adults and children hospitalized in the United States: a propensity analysis. Clin Infect Dis. 2005;41:1232–9. - PubMed
-
- Fridkin SK. Candidemia is costly—plain and simple. Clin Infect Dis. 2005;41:1240–1. - PubMed
-
- Morgan JMD, Meltzer MIP, Plikaytis BDM, et al. Excess mortality, hospital stay, and cost due to candidemia: a case-control study using data from population-based candidemia surveillance. Infect Control Hosp Epidemiol. 2005;26:540–7. - PubMed
-
- Gudlaugsson O, Gillespie S, Lee K, et al. Attributable mortality of nosocomial candidemia, revisited. Clin Infect Dis. 2003;37:1172–7. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
