

Risk factors for vitamin D deficiency and relationship with cardiac biomarkers, inflammation and immune restoration in HIV-infected youth
- PMID: 22894927
- PMCID: PMC3717313
- DOI: 10.3851/IMP2318
Risk factors for vitamin D deficiency and relationship with cardiac biomarkers, inflammation and immune restoration in HIV-infected youth
Abstract
Background: Vitamin D deficiency is common in HIV-infected individuals. In adults, traditional and HIV-related factors play a role in vitamin D status, and deficiency appears to impair immune restoration and exacerbate HIV complications, like cardiovascular disease (CVD). This study sought to determine factors contributing to vitamin D status in HIV-infected youth and investigate the relationship with CVD risk, inflammation and immune restoration.
Methods: HIV-infected subjects (1-25 years old) were enrolled prospectively along with healthy controls that were group-matched by age, sex and race. HIV data were collected for the HIV-infected group, while traditional risk factors, including vitamin D intake, sun exposure, skin pigmentation, physical activity level and body mass index (BMI) were collected for both groups. Fasting lipids, plasma 25-hydroxyvitamin D (25[OH]D), and inflammation markers were measured.
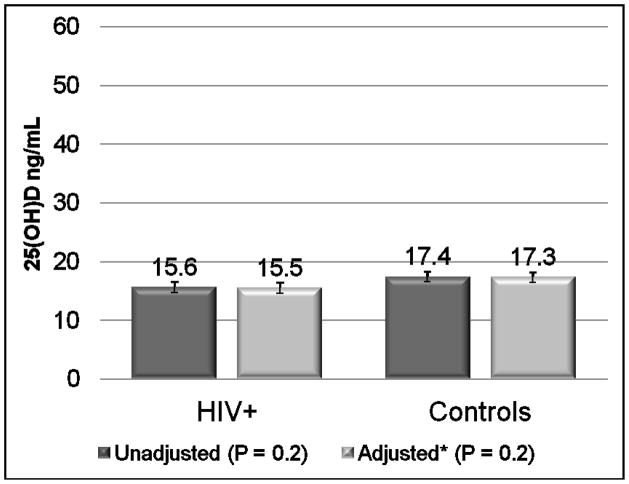
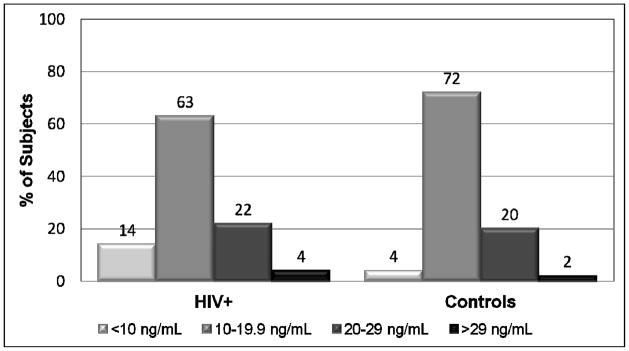
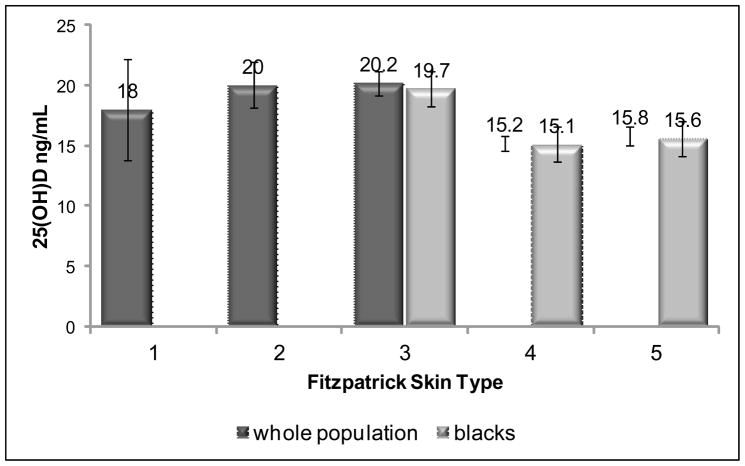
Results: In total, 200 HIV-infected subjects and 50 controls were enrolled. HIV group had 53% male, 95% Black and a mean age of 17.2 ±4.6 years. There was no difference in 25(OH)D between groups; 77% of HIV+ and 74% of controls had 25(OH)D<20 ng/ml. Only Fitzpatrick skin type was independently associated with 25(OH)D. No HIV variables were associated with 25(OH)D, even when HIV sub-populations were examined. Inflammation, CVD risk factors and immune restoration were not independently associated with 25(OH)D.
Conclusions: Vitamin D deficiency is common among HIV-infected youth. However, HIV factors, CVD risk, inflammation and immune restoration do not appear to have the same relationship with vitamin D as has been shown in adults. Supplementation trials are needed to determine if increasing 25(OH)D concentrations could better elucidate these relationships.
Conflict of interest statement
Figures
References
-
- Stephensen CB, Marquis GS, Kruzich LA, Douglas SD, Aldrovandi GM, Wilson CM. Vitamin D status in adolescents and young adults with HIV infection. American Journal of Clinical Nutrition. 2006;83:1135–1141. - PubMed
-
- Rutstein R, Downes A, Zemel B, Schall J, Stallings V. Vitamin D status in children and young adults with perinatally acquired HIV infection. Clin Nutr. 2011;30:624–628. - PubMed
-
- Giovannucci E. Vitamin D status and cancer incidence and mortality. Advances in Experimental Medicine & Biology. 2008;624:31–42. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
