

Short-term late-generation antibiotics versus longer term penicillin for acute streptococcal pharyngitis in children
- PMID: 22895944
- PMCID: PMC11984625
- DOI: 10.1002/14651858.CD004872.pub3
Short-term late-generation antibiotics versus longer term penicillin for acute streptococcal pharyngitis in children
Abstract
Background: The standard duration of treatment for children with acute group A beta hemolytic streptococcus (GABHS) pharyngitis with oral penicillin is 10 days. Shorter duration antibiotics may have comparable efficacy.
Objectives: To summarize the evidence regarding the efficacy of two to six days of newer oral antibiotics (short duration) compared to 10 days of oral penicillin (standard duration) in treating children with acute GABHS pharyngitis.
Search methods: We searched the Cochrane Central Register of Controlled Trials (CENTRAL 2012, Issue 3) which contains the Cochrane Acute Respiratory Infections Group's Specialized Register, MEDLINE (January 1966 to March week 3, 2012) and EMBASE (January 1990 to April 2012).
Selection criteria: Randomized controlled trials (RCTs) comparing short duration oral antibiotics to standard duration oral penicillin in children aged 1 to 18 years with acute GABHS pharyngitis.
Data collection and analysis: Two review authors scanned the titles and abstracts of retrieved citations and applied the inclusion criteria. We retrieved included studies in full, and extracted data. Two review authors independently assessed trial quality.
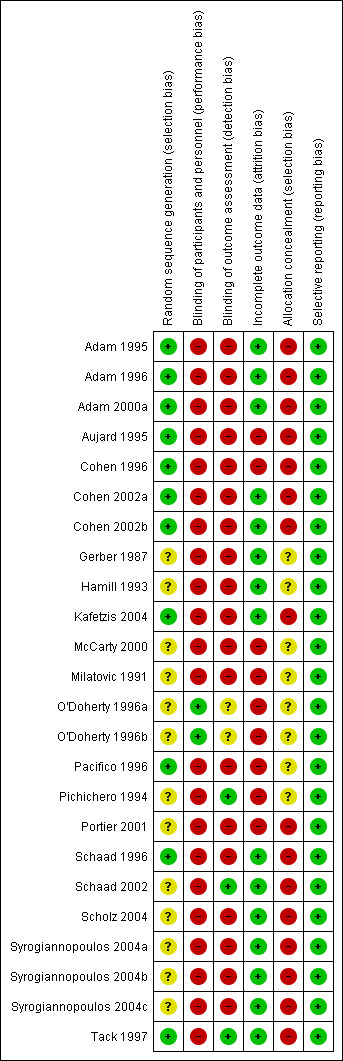
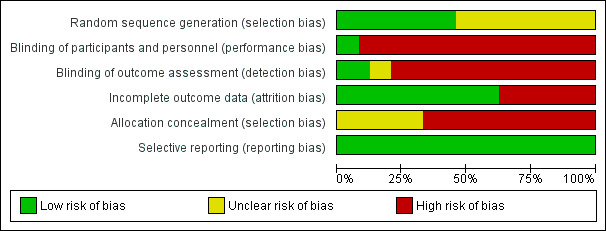
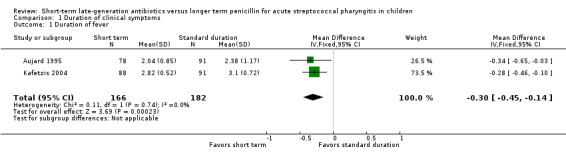
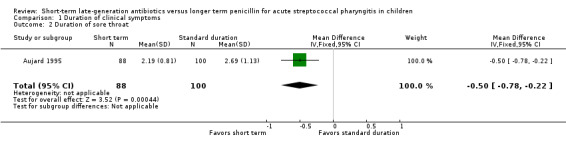
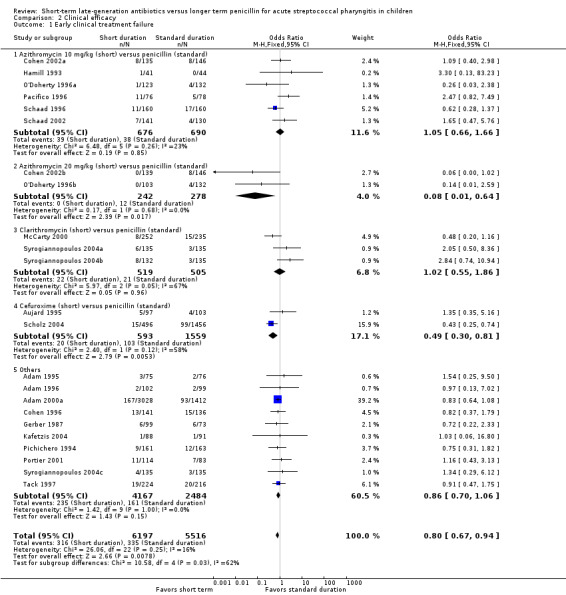
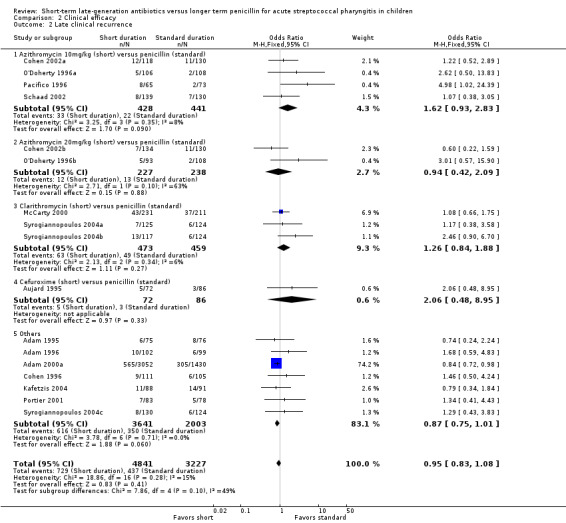
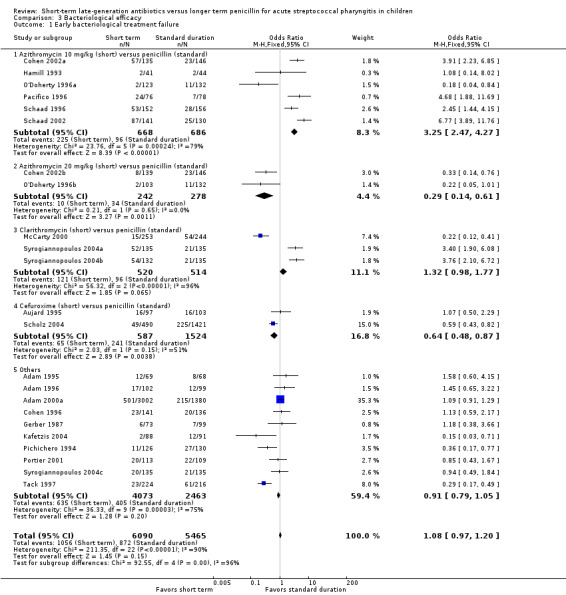
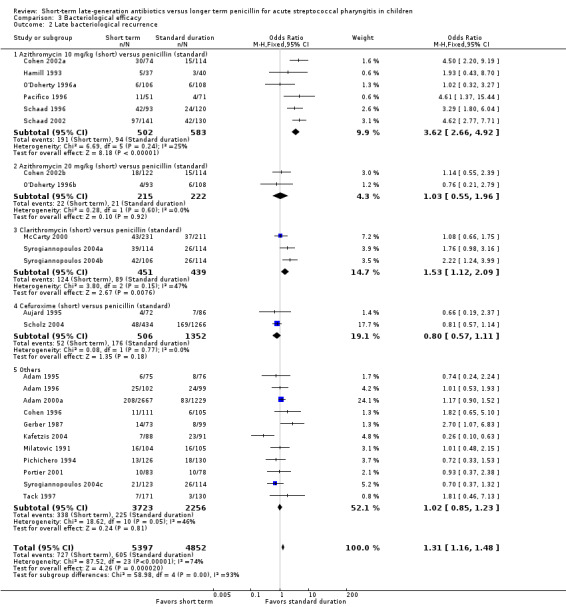
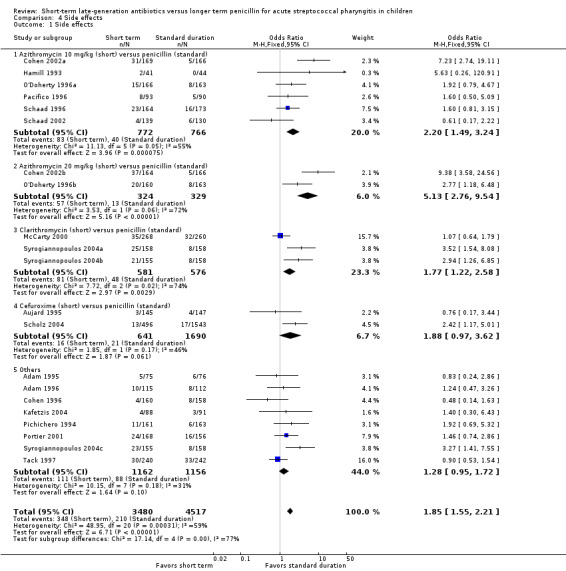
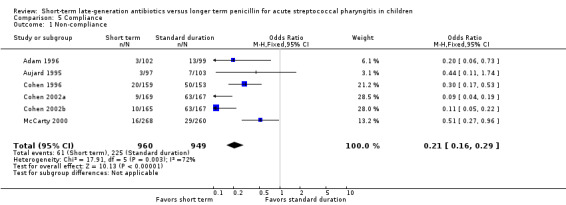
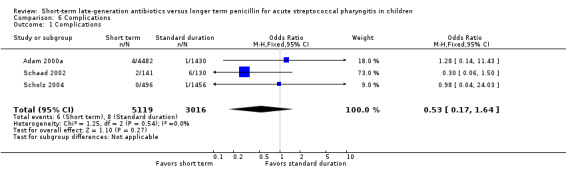
Main results: We included 20 studies with 13,102 cases of acute GABHS pharyngitis. The updated search did not identify any new eligible studies; the majority of studies were at high risk of bias. However, the majority of the results were consistent. Compared to standard duration treatment, the short duration treatment studies had shorter periods of fever (mean difference (MD) -0.30 days, 95% confidence interval (CI) -0.45 to -0.14) and throat soreness (MD -0.50 days, 95% CI -0.78 to -0.22); lower risk of early clinical treatment failure (odds ratio (OR) 0.80, 95% CI 0.67 to 0.94); no significant difference in early bacteriological treatment failure (OR 1.08, 95% CI 0.97 to 1.20) or late clinical recurrence (OR 0.95, 95% CI 0.83 to 1.08). However, the overall risk of late bacteriological recurrence was worse in the short duration treatment studies (OR 1.31, 95% CI 1.16 to 1.48), although no significant differences were found when studies of low dose azithromycin (10 mg/kg) were eliminated (OR 1.06, 95% CI 0.92 to 1.22). Three studies reported long duration complications. Out of 8135 cases of acute GABHS pharyngitis, only six cases in the short duration treatment versus eight in the standard duration treatment developed long-term complications in the form of glomerulonephritis and acute rheumatic fever, with no statistically significant difference (OR 0.53, 95% CI 0.17 to 1.64).
Authors' conclusions: Three to six days of oral antibiotics had comparable efficacy compared to the standard duration 10-day course of oral penicillin in treating children with acute GABHS pharyngitis. . In areas where the prevalence of rheumatic heart disease is still high, our results must be interpreted with caution.
Conflict of interest statement
None known.
Figures
Update of
-
Short versus standard duration antibiotic therapy for acute streptococcal pharyngitis in children.Cochrane Database Syst Rev. 2009 Jan 21;(1):CD004872. doi: 10.1002/14651858.CD004872.pub2. Cochrane Database Syst Rev. 2009. Update in: Cochrane Database Syst Rev. 2012 Aug 15;(8):CD004872. doi: 10.1002/14651858.CD004872.pub3. PMID: 19160243 Updated.
Comment in
-
Are short-term late-generation antibiotics equivalent to standard penicillin therapy in the resolution of symptoms in acute strep throat in children?Ann Emerg Med. 2014 Jun;63(6):690-1. doi: 10.1016/j.annemergmed.2013.09.023. Epub 2013 Oct 23. Ann Emerg Med. 2014. PMID: 24161837 No abstract available.
-
Short-term oral antibiotics may be as effective as the standard course of penicillin for children with acute streptococcal pharyngitis.J Am Dent Assoc. 2015 Dec;146(12):927-8. doi: 10.1016/j.adaj.2015.09.017. J Am Dent Assoc. 2015. PMID: 26610839 No abstract available.
References
References to studies included in this review
Adam 1995 {published data only}
-
- Adam D, Hostalek U, Troster K, Cefixim Study Group. 5‐day cefixim therapy for bacterial pharyngitis and/or tonsillitis: comparison with 10 day penicillin V therapy. Infection 1995;23(Suppl 2):83‐6. - PubMed
Adam 1996 {published data only}
-
- Adam D, Scholz H, Pharyngitis Study Group. Five days of erythromycin estolate versus ten days of penicillin V in the treatment of group A streptococcal tonsillopharyngitis in children. European Journal of Clinical Microbiology and Infectious Diseases 1996;15:712‐7. - PubMed
Adam 2000a {published data only}
-
- Adam D, Schoz H, Helmerking M. Short‐course antibiotic treatment of 4782 culture‐proven cases of group A streptococcal tonsillopharyngitis and incidence of poststreptococcal sequelae. Journal of Infectious Diseases 2000;182(2):509‐16. - PubMed
Aujard 1995 {published data only}
-
- Aujard Y, Boucot I, Brahimi N, Chiche D, Bingen E. Comparative efficacy and safety of four‐day cefuroxime axetil and ten‐day penicillin treatment of group A beta‐hemolytic streptococcal pharyngitis in children. Pediatric Infectious Disease Journal 1995;14(4):295‐300. - PubMed
Cohen 1996 {published data only}
-
- Cohen R, Levy C, Doit C, Rocque F, Boucherat M, Fitoussi F, et al. Six‐day amoxicillin vs ten‐day penicillin V therapy for group A streptococcal tonsillopharyngitis. Pediatric Infectious Disease Journal 1996;15(8):678‐82. - PubMed
Cohen 2002a {published data only}
-
- Cohen R, Reinert P, Rocque F, Levy C, Boucherat M, Robert M, et al. Comparison of two dosages of azithromycin for three days versus penicillin V for ten days in acute group A streptococcal tonsillopharyngitis. Pediatric Infectious Disease Journal 2002;21(4):297‐303. - PubMed
Cohen 2002b {published data only}
-
- Cohen R, Reinert P, Rocque F, Levy C, Boucherat M, Robert M, et al. Comparison of two dosages of azithromycin for three days versus penicillin V for ten days in acute group A streptococcal tonsillopharyngitis. Pediatric Infectious Disease Journal 2002;21(4):297‐303. - PubMed
Gerber 1987 {published data only}
-
- Gerber MA, Randolph MF, Chanatry J, Wright LL, Meo K, Kaplan EL. Five versus ten days of penicillin V therapy for streptococcal pharyngitis. American Journal of Diseases in Children 1987;141(2):224‐7. - PubMed
Hamill 1993 {published data only}
-
- Hamill J. Mulicenter evaluation of azithromycin and penicillin V in the treatment of acute streptococcal pharyngitis and tonsillitis in children. Journal of Antimicrobial Chemotherapy 1993;31(Suppl E):89‐94. - PubMed
Kafetzis 2004 {published data only}
-
- Kafetzis D, Liapi G, Tsolia M, Aoudi H, Mathioudakis J, Paraskakis I, et al. Failure to eradicate group A beta‐hemolytic streptococci (GABHS) from the upper respiratory tract after antibiotic treatment. International Journal of Antimicrobial Agents 2004;23(1):67‐71. - PubMed
McCarty 2000 {published data only}
-
- McCarty J, Hedrick J, Gooch W. Clarithromycin suspension versus penicillin V suspension in children with streptococcal pharyngitis. Advance in Therapy 2000;17(1):14‐26. - PubMed
Milatovic 1991 {published data only}
-
- Milatovic D. Evaluation of cefadroxil, penicillin and erythromycin in the treatment of streptococcal tonsillopharyngitis. Pediatric Infectious Disease Journal 1991;10(Suppl 10):61‐3. - PubMed
O'Doherty 1996a {published data only}
-
- O'Doherty B, Paediatric Azithromycin Study Group. Azithromycin versus penicillin V in the treatment of paediatric patients with acute streptococcal pharyngitis/tonsillitis. European Journal of Clinical Microbiology and Infectious Diseases 1996;15(9):718‐24. - PubMed
O'Doherty 1996b {published data only}
-
- O'Doherty B, Paediatric Azithromycin Study Group. Azithromycin versus penicillin V in the treatment of paediatric patients with acute streptococcal pharyngitis/tonsillitis. European Journal of Clinical Microbiology and Infectious Diseases 1996;15(9):718‐24. - PubMed
Pacifico 1996 {published data only}
Pichichero 1994 {published data only}
-
- Pichichero M, Gooch W, Rodriguez W, Blumer J, Aronoff S, Jacobs R, et al. Effective short‐course treatment of acute group A beta hemolytic streptococcal tonsillopharyngitis. Archives of Pediatrics and Adolesent Medicine 1994;148(10):1053‐60. - PubMed
Portier 2001 {published data only}
-
- Portier H, Bourrillon A, Lucht F, Choutet P, Gehanno P, Meziane L, et al. Treatment of acute group A beta‐hemolytic streptococcal tonsillitis in children with 5‐day course of josamycine [Treatment des angines aigues a' strptocoque beta he'molytique du groupe A chez I enfant per la josamycine pendant cinq jours]. Archives de Pediatrie 2001;8:700‐6. - PubMed
Schaad 1996 {published data only}
-
- Schaad U, Heynen G, Swiss Tonsillopharyngitis Study Group. Evaluation of the efficacy, safety and toleration of azithromycin vs penicillin V in the treatment of acute streptococcal pharyngitis in children: results of multicenter, open comparative study. Pediatric Infectious Disease Journal 1996;15(9):791‐5. - PubMed
Schaad 2002 {published data only}
-
- Schaad U, Kellerhals P, Altwegg M, Swiss Pharyngitis Study Group. Azithromycin versus penicillin V for treatment of acute group A streptococcal pharyngitis. Pediatric Infectious Disease Journal 2002;21(4):304‐8. - PubMed
Scholz 2004 {published data only}
-
- Scholz H. Streptococcal‐A tonsillopharyngitis: a 5‐day course of cefuroxime axetil versus a 10‐day course of penicillin V. Chemotherapy 2004;50:51‐4. - PubMed
Syrogiannopoulos 2004a {published and unpublished data}
-
- Syrogiannopoulos G, Bozdogan B, Grivea I, Ednie L, Kritikou D, Katopodis G, et al. Hellenic Antibiotic‐Resistant Respiratory Pathogens Study Group. Two dosages of clarithromycine for five days, amoxacillin/clavulanate for five days or penicillin V for ten days in acute group A streptococcal tonsillopharyngitis. Pediatric Infectious Disease Journal 2004;23(9):857‐65. - PubMed
Syrogiannopoulos 2004b {published data only}
-
- Syrogiannopoulos G. Two dosages of clarithromycin for five days, amoxicillin/clavulanate for five days or penicillin V for ten days in acute group A streptococcal tonsillopharyngitis. Pediatric Infectious Disease Journal 2004;23(9):857‐65. - PubMed
Syrogiannopoulos 2004c {published data only}
-
- Syrogiannopoulos G. Two dosages of clarithromycin for five days, amoxicillin/clavulanate for five days or penicillin V for ten days in acute group A streptococcal tonsillopharyngitis. Pediatric Infectious Disease Journal 2004;23(9):857‐65. - PubMed
Tack 1997 {published data only}
-
- Tack K, Hedrick J, Rothstien E, Nemeth MA, Keyserling C, Pichichero M, et al. A study of 5‐day cefdinir treatment for streptococcal pharyngitis in children. Archives of Pediatrics and Adolescent Medicine 1997;151(1):45‐9. - PubMed
References to studies excluded from this review
Adam 2000b {published data only}
-
- Adam D, Scholz H, Helmerking M. Comparison of short‐course (5 days) cefuroxime axetil with a standard 10 day oral penicillin V regimen in the treatment of tonsillopharyngitis. Journal of Antimicrobial Chemotherapy 2000;45:23‐30. - PubMed
Additional references
Bisno 1997
Carapetis 2005
-
- Carapetis JR, Steer AC, Mulholland EK, Weber M. The global burden of group A streptococcal diseases. Lancet Infectious Diseases 2005;5:685‐94. - PubMed
Chalmers 1981
-
- Chalmers TC, Smith H Jr, Blackburn B, Silverman B, Schroeder B, Rietman D, et al. A method for assessing the quality of a randomized clinical trial. Controlled Clinical Trials 1981;2:31‐49. - PubMed
Higgins 2011
-
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Kumar 2008
-
- Kumar V, Fausto N, Abbas A. Robbins and Cotran Pathologic Basis of Disease. 7th Edition. Philadelphia: Elsevier, 2008.
Lefebvre 2011
-
- Lefebvre C, Manheimer E, Glanville J. Chapter 6: Searching for studies. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Meade 1997
-
- Meade MO, Richardson WS. Selecting and appraising studies for a systematic review. Annals of Internal Medicine 1997;127:531‐7. - PubMed
Nandi 2001
Olivier 2000
-
- Olivier C. Rheumatic fever: is it still a problem?. Journal of Antimicrobial Chemotherapy 2000;45:13‐21. - PubMed
Shulman 2006
-
- Shulman ST, Stollerman G, Beall B, Dale JB, Tanz RR. Temporal changes in streptococcal M protein types and the near‐disappearance of acute rheumatic fever in the United States. Clinical Infectious Diseases 2006;15:441‐7. - PubMed
Spinks 2011
Thornton 2000
-
- Thornton A, Lee P. Publication bias in meta‐analysis: its causes and consequences. Journal of Clinical Epidemiology 2000;53:207‐16. - PubMed
References to other published versions of this review
Altamimi 2009
Altamimi 2010
-
- Altamimi S, Khalil A, Khalaiwi KA, Milner R, Pusic M, Al Othman MA. Short versus standard duration antibiotic therapy for acute streptococcal pharyngitis in children. Sao Paulo Medical Journal 2010;128(1):48. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous