

Different intensities of glycaemic control for pregnant women with pre-existing diabetes
- PMID: 22895976
- PMCID: PMC4164477
- DOI: 10.1002/14651858.CD008540.pub3
Different intensities of glycaemic control for pregnant women with pre-existing diabetes
Update in
-
Different intensities of glycaemic control for pregnant women with pre-existing diabetes.Cochrane Database Syst Rev. 2016 May 4;2016(5):CD008540. doi: 10.1002/14651858.CD008540.pub4. Cochrane Database Syst Rev. 2016. PMID: 27142841 Free PMC article.
Abstract
Background: The optimal glycaemic control target in pregnant women with pre-existing diabetes is unclear, although there is a clear link between high glucose concentrations and adverse birth outcomes.
Objectives: To assess the effects of different intensities of glycaemic control in pregnant women with pre-existing type 1 or type 2 diabetes.
Search methods: We searched the Cochrane Pregnancy and Childbirth Group's Trials Register (30 April 2012).
Selection criteria: We included randomised controlled trials comparing different glycaemic control targets in pregnant women with pre-existing diabetes.
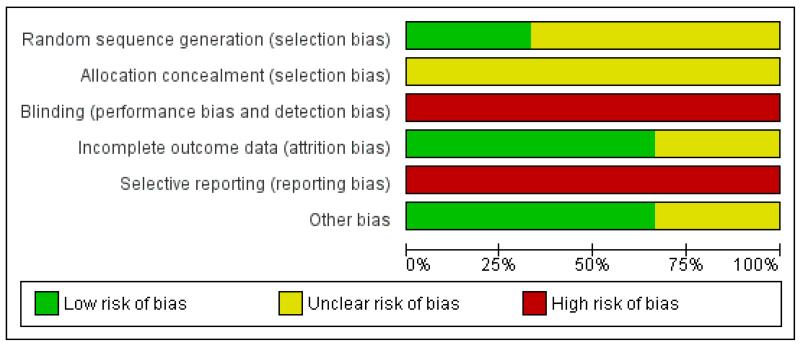
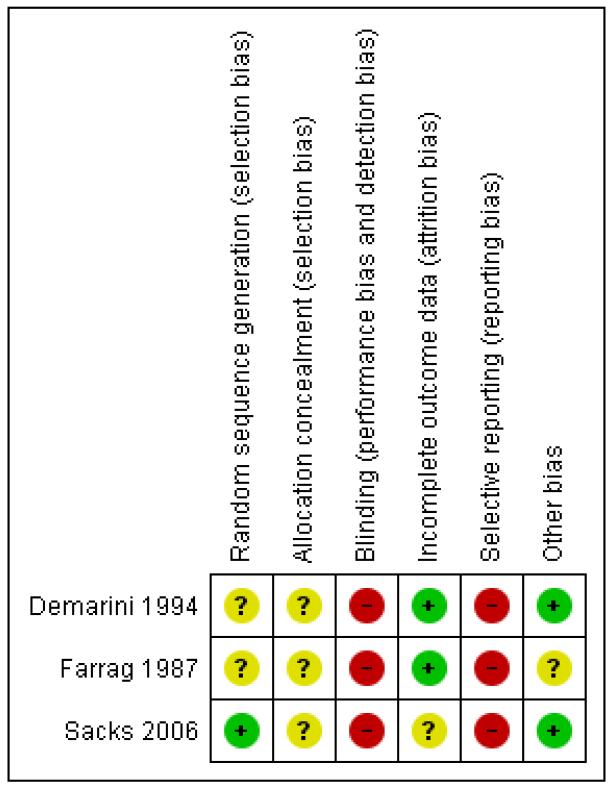
Data collection and analysis: Two review authors assessed trial eligibility and risk of bias, and extracted data.
Main results: We included three trials all in women with type 1 diabetes (223 women and babies), and all with a high risk of bias. Two trials compared very tight (3.33 to 5.0 mmol/L fasting blood glucose (FBG)) with tight-moderate (4.45 to 6.38) glycaemic control targets, with one trial of 22 babies reporting no perinatal deaths or serious perinatal morbidity. In the same trial, there were two birth defects in the very tight and none in the tight-moderate group with no significant differences in caesarean section between groups (risk ratio 0.92, 95% confidence interval (CI) 0.49 to 1.73). In these two trials glycaemic control was not significantly different between the very tight and tight-moderate groups by the third trimester, although one trial of 22 women found significantly less maternal hypoglycaemia in the tight-moderate group.In a trial of 60 women and babies comparing tight (≤ 5.6 mmol/L FBG); moderate (5.6 to 6.7); and loose (6.7 to 8.9) glycaemic control targets, there were two neonatal deaths in the loose and none in the tight or moderate groups. There were significantly fewer women with pre-eclampsia, fewer caesareans and fewer birthweights greater than 90th centile in the combined tight-moderate compared with the loose group.
Authors' conclusions: In a very limited body of evidence, few differences in outcomes were seen between very tight and tight-moderate glycaemic control targets in pregnant women with pre-existing type 1 diabetes, including actual glycaemic control achieved. There is evidence of harm (increased pre-eclampsia, caesareans and birthweights greater than 90th centile) for 'loose' control (FBG above 7 mmol/L). Future trials comparing interventions, rather than glycaemic control targets, may be more feasible particularly for pregnant women with type 2 diabetes.
Figures
Update of
-
Different intensities of glycaemic control for pregnant women with pre-existing diabetes.Cochrane Database Syst Rev. 2010 Sep 8;(9):CD008540. doi: 10.1002/14651858.CD008540.pub2. Cochrane Database Syst Rev. 2010. Update in: Cochrane Database Syst Rev. 2012 Aug 15;(8):CD008540. doi: 10.1002/14651858.CD008540.pub3. PMID: 20824880 Updated.
References
References to studies included in this review
-
- Demarini S, Mimouni F, Tsang RC, Khoury J, Hertzberg V. Impact of metabolic control of diabetes during pregnancy on neonatal hypocalcemia: a randomized study. Obstetrics and Gynecology. 1994;83(6):918–22. - PubMed
- Mimouni F, Miodovnik M, Whitsett JA, Holyroyde JC, Siddiqi TA, Tsang RC. Respiratory distress syndrome in infants of diabetic mothers in the 1980s: no direct adverse effect of maternal diabetes with modern management. Obstetrics and Gynecology. 1987;69:191–5. - PubMed
-
- Farrag OAM. Prospective study of 3 metabolic regimens in pregnant diabetes. Australian and New Zealand Journal of Obstetrics and Gynaecology. 1987;27:6–9. - PubMed
-
- Sacks DA, Feig DS, Liu Ai-L, Wolde-Tsadik G. Managing type 1 diabetes in pregnancy: how near normal is necessary? Journal of Perinatology. 2006;26:458–62. - PubMed
References to studies excluded from this review
-
- The Diabetes Control and Complications Trial Research Group Effect of pregnancy on microvascular complications in the Diabetes Control and Complications Trial. Diabetes Care. 2000;23(8):1084–91. - PMC - PubMed
- The Diabetes Control and Complications Trial Research Group Pregnancy outcomes in the Diabetes Control and Complications Trial. American Journal of Obstetrics and Gynecology. 1996;174(4):1343–53. - PubMed
Additional references
-
- ACOG Pregestational diabetes mellitus: ACOG Practice Bulletin Number 60. Obstetrics & Gynecology. 2005;105(3):675–85. - PubMed
-
- [accessed 2009];The Australasian Diabetes in Pregnancy Society consensus guidelines for the management of patients with type 1 and type 2 diabetes in relation to pregnancy. 2005 www.adips.org/content/ADIPS.PreGDM.Guidelines.pdf. - PubMed
-
- Balsells M, Garcia-Patterson A, Gich I, Corcoy R. Maternal and fetal outcome in women with type 2 versus type 1 diabetes: a systematic review and metaanalysis. Journal of Clinical Endocrinology and Metabolism. 2009;94(11):4284–91. - PubMed
-
- Bell R, Bailey K, Cresswell T, Hawthorne G, Critchley J, Lewis-Barned N, on behalf of the Northern Diabetic Pregnancy Survey Steering Group Trends in prevalence and outcomes of pregnancy in women with pre-existing type I and type II diabetes. BJOG: an international journal of obstetrics and gynaecology. 2008;115(4):445–52. - PubMed
References to other published versions of this review
-
- Middleton P, Crowther CA, Simmonds L, Muller P. Different intensities of glycaemic control for pregnant women with pre-existing diabetes. Cochrane Database of Systematic Reviews. 2010;(Issue 9) [DOI: 10.1002/ 14651858.CD008540.pub2] - PubMed
-
-
* Indicates the major publication for the study
-
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous