

Ergonomic design and training for preventing work-related musculoskeletal disorders of the upper limb and neck in adults
- PMID: 22895977
- PMCID: PMC6486299
- DOI: 10.1002/14651858.CD008570.pub2
Ergonomic design and training for preventing work-related musculoskeletal disorders of the upper limb and neck in adults
Update in
-
Ergonomic interventions for preventing work-related musculoskeletal disorders of the upper limb and neck among office workers.Cochrane Database Syst Rev. 2018 Oct 23;10(10):CD008570. doi: 10.1002/14651858.CD008570.pub3. Cochrane Database Syst Rev. 2018. PMID: 30350850 Free PMC article.
Abstract
Background: Work-related upper limb and neck musculoskeletal disorders (MSDs) are one of the most common occupational disorders around the world. Although ergonomic design and training are likely to reduce the risk of workers developing work-related upper limb and neck MSDs, the evidence is unclear.
Objectives: To assess the effects of workplace ergonomic design or training interventions, or both, for the prevention of work-related upper limb and neck MSDs in adults.
Search methods: We searched MEDLINE, EMBASE, the Cochrane Central Register of Controlled Trials (CENTRAL), CINAHL, AMED, Web of Science (Science Citation Index), SPORTDiscus, Cochrane Occupational Safety and Health Review Group Database and Cochrane Bone, Joint and Muscle Trauma Group Specialised Register to July 2010, and Physiotherapy Evidence Database, US Centers for Disease Control and Prevention, the National Institute for Occupational Safety and Health database, and International Occupational Safety and Health Information Centre database to November 2010.
Selection criteria: We included randomised controlled trials (RCTs) of ergonomic workplace interventions for preventing work-related upper limb and neck MSDs. We included only studies with a baseline prevalence of MSDs of the upper limb or neck, or both, of less than 25%.
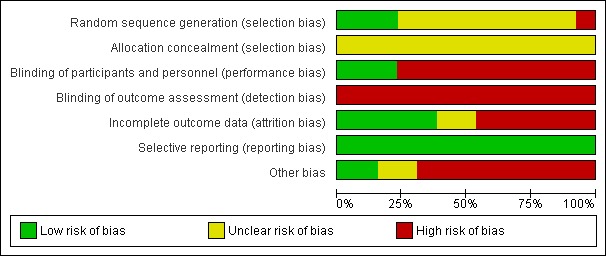
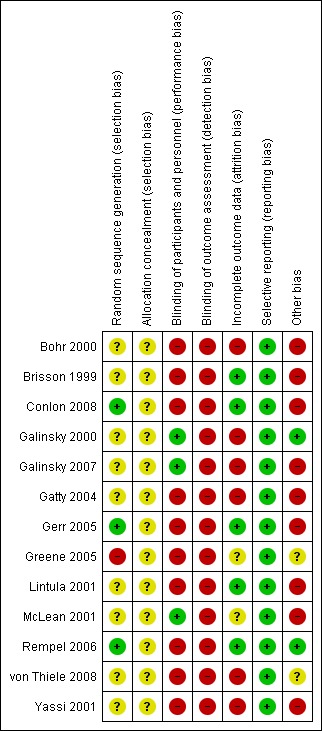
Data collection and analysis: Two review authors independently extracted data and assessed risk of bias. We included studies with relevant data that we judged to be sufficiently homogeneous regarding the intervention and outcome in the meta-analysis. We assessed the overall quality of the evidence for each comparison using the GRADE approach.
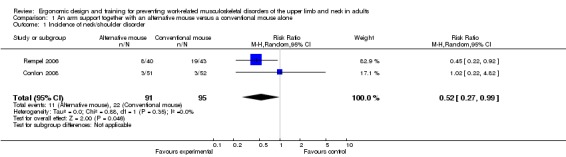
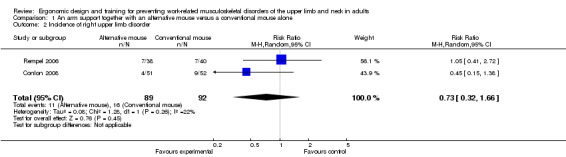
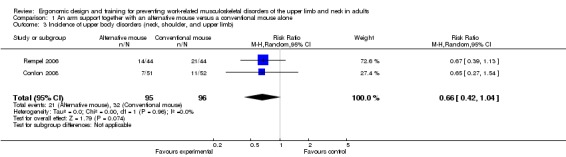
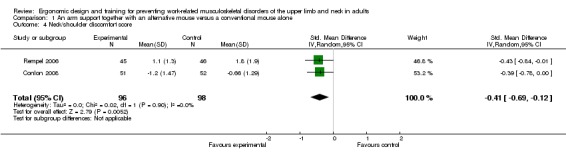
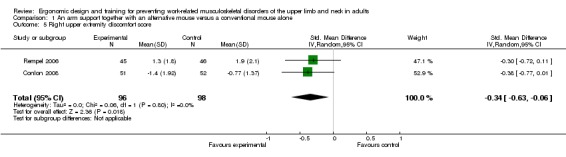
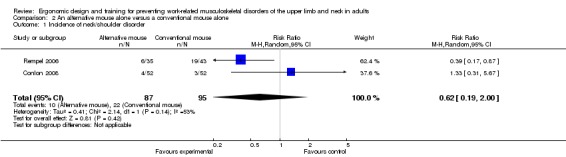
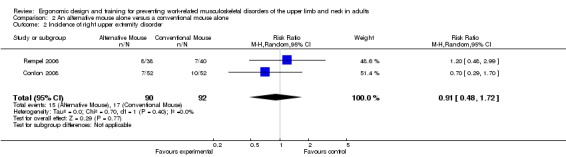
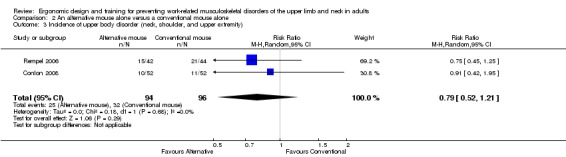
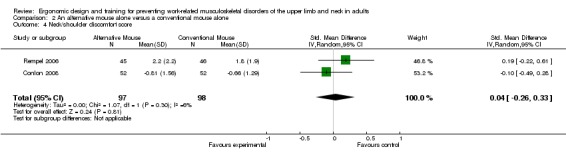
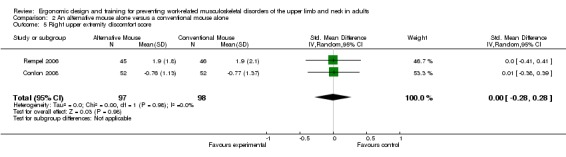
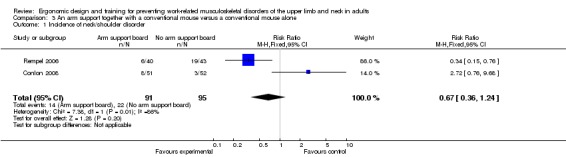
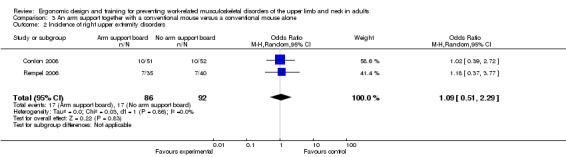
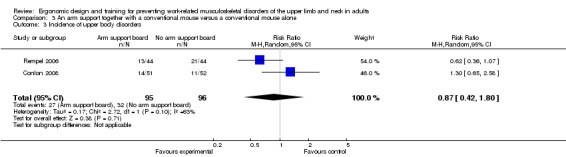
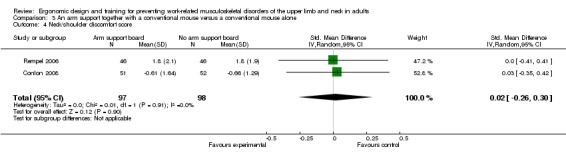
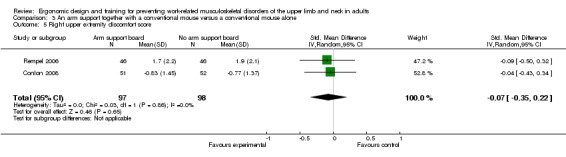
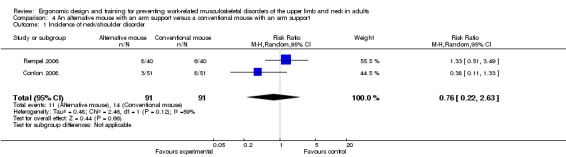
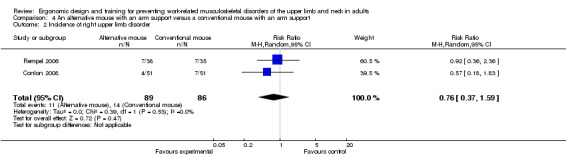
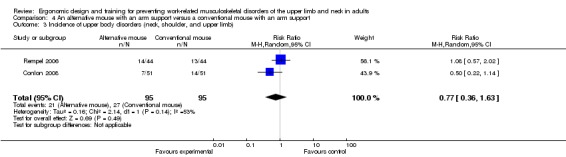
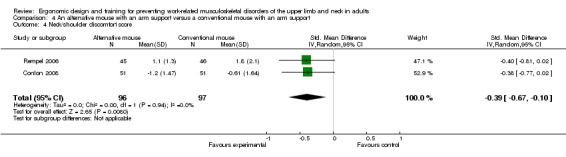
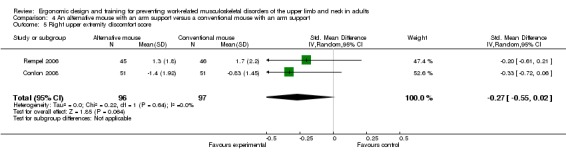
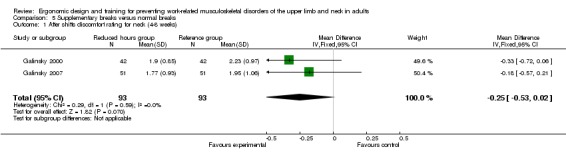
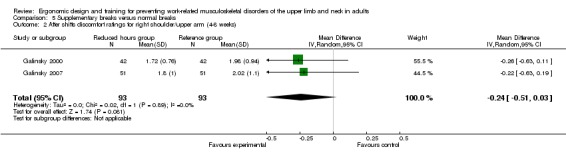
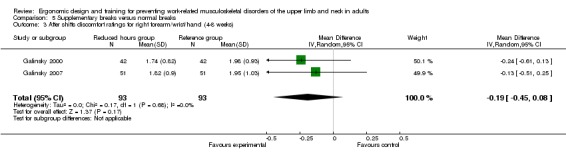
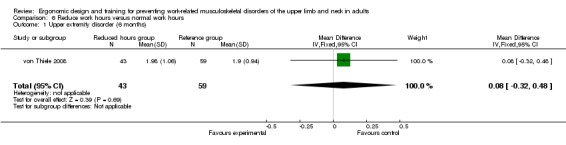
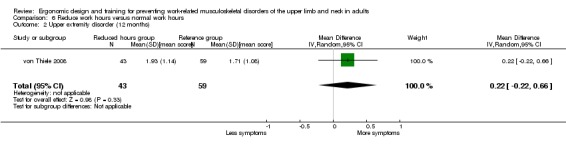
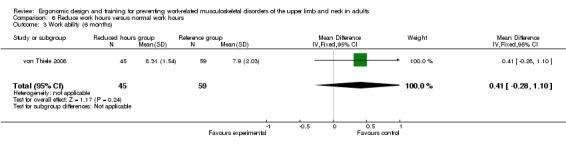
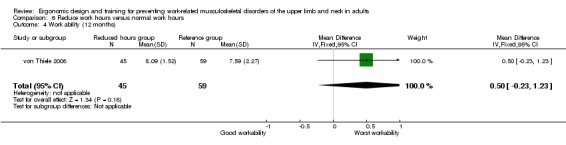
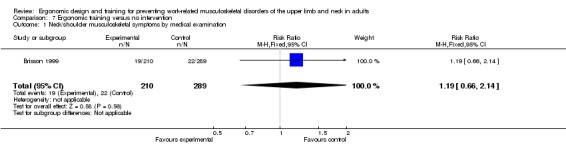
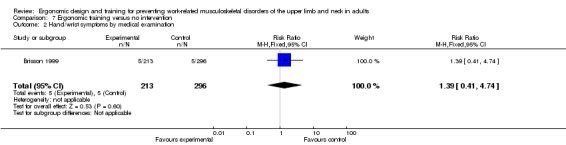
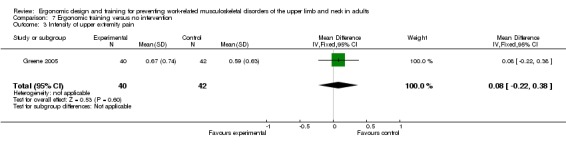
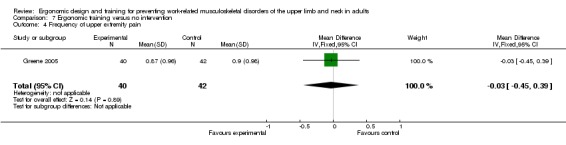
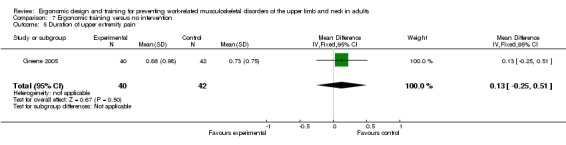
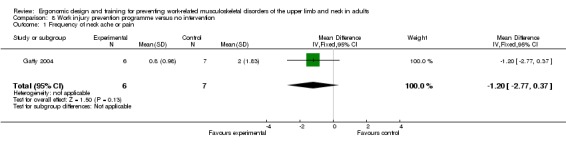
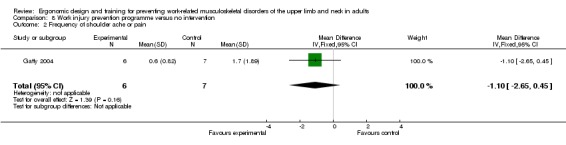
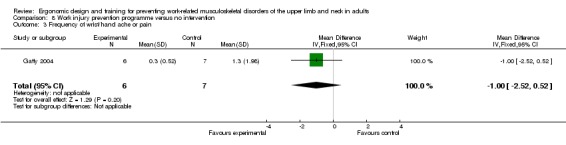
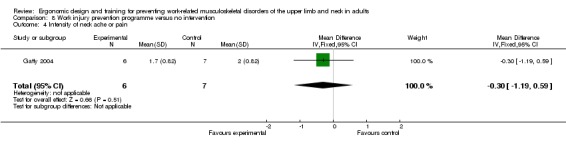
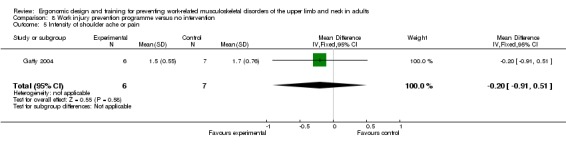
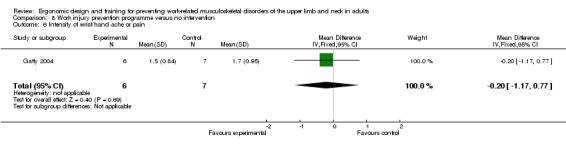
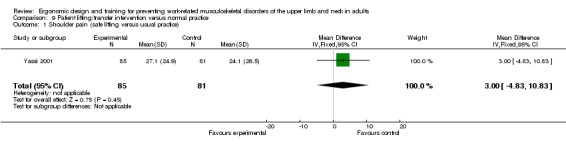
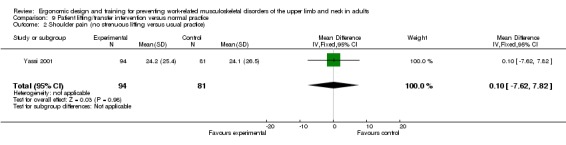
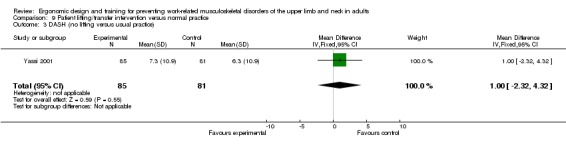
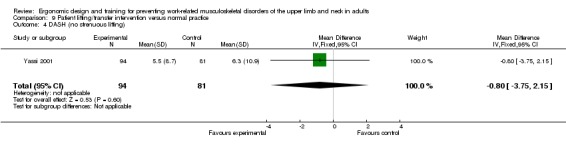
Main results: We included 13 RCTs (2397 workers). Eleven studies were conducted in an office environment and two in a healthcare setting. We judged one study to have a low risk of bias. The 13 studies evaluated effectiveness of ergonomic equipment, supplementary breaks or reduced work hours, ergonomic training, a combination of ergonomic training and equipment, and patient lifting interventions for preventing work-related MSDs of the upper limb and neck in adults.Overall, there was moderate-quality evidence that arm support with alternative mouse reduced the incidence of neck/shoulder disorders (risk ratio (RR) 0.52; 95% confidence interval (CI) 0.27 to 0.99) but not the incidence of right upper limb MSDs (RR 0.73; 95% CI 0.32 to 1.66); and low-quality evidence that this intervention reduced neck/shoulder discomfort (standardised mean difference (SMD) -0.41; 95% CI -0.69 to -0.12) and right upper limb discomfort (SMD -0.34; 95% CI -0.63 to -0.06).There was also moderate-quality evidence that the incidence of neck/shoulder and right upper limb disorders were not reduced when comparing alternative mouse and conventional mouse (neck/shoulder RR 0.62; 95% CI 0.19 to 2.00; right upper limb RR 0.91; 95% CI 0.48 to 1.72), arm support and no arm support with conventional mouse (neck/shoulder RR 0.67; 95% CI 0.36 to 1.24; right upper limb RR 1.09; 95% CI 0.51 to 2.29), and alternative mouse with arm support and conventional mouse with arm support (neck/shoulder RR 0.58; 95% CI 0.30 to 1.12; right upper limb RR 0.92; 95% CI 0.36 to 2.36).There was low-quality evidence that using an alternative mouse with arm support compared to conventional mouse with arm support reduced neck/shoulder discomfort (SMD -0.39; 95% CI -0.67 to -0.10). There was low- to very low-quality evidence that other interventions were not effective in reducing work-related upper limb and neck MSDs in adults.
Authors' conclusions: We found moderate-quality evidence to suggest that the use of arm support with alternative mouse may reduce the incidence of neck/shoulder MSDs, but not right upper limb MSDs. Moreover, we found moderate-quality evidence to suggest that the incidence of neck/shoulder and right upper limb MSDs is not reduced when comparing alternative and conventional mouse with and without arm support. However, given there were multiple comparisons made involving a number of interventions and outcomes, high-quality evidence is needed to determine the effectiveness of these interventions clearly. While we found very-low- to low-quality evidence to suggest that other ergonomic interventions do not prevent work-related MSDs of the upper limb and neck, this was limited by the paucity and heterogeneity of available studies. This review highlights the need for high-quality RCTs examining the prevention of MSDs of the upper limb and neck.
Conflict of interest statement
None known.
Figures
References
References to studies included in this review
-
- Bohr PC. Efficacy of office ergonomics education. Journal of Occupational Rehabilitation 2000;10(4):243‐55.
-
- Brisson C, Montreuil S, Punnett L. Effects of an ergonomic training program on workers with video display units. Scandinavian Journal of Work, Environment and Health 1999;25(3):255‐63. - PubMed
-
- Conlon CF, Krause N, Rempel DM. A randomised controlled trial evaluating an alternative mouse and forearm support on upper body discomfort and musculoskeletal disorders among engineers. Occupational and Environmental Medicine 2008;65(5):311‐8. - PubMed
- Conlon CF, Krause N, Rempel DM. A randomized controlled trial evaluating an alternative mouse or forearm support on change in median and ulnar nerve motor latency at the wrist. American Journal of Industrial Medicine 2009;52(4):304‐10. - PubMed
-
- Galinsky TL, Swanson NG, Sauter SL, Hurrell JJ, Schleifer LM. A field study of supplementary rest breaks for data‐entry operators. Ergonomics 2000;43(5):622‐38. - PubMed
-
- Galinsky T, Swanson N, Sauter S, Dunkin R, Hurrell J, Schleifer L. Supplementary breaks and stretching exercises for data entry operators: a follow‐up field study. American Journal of Industrial Medicine 2007;50(7):519‐27. - PubMed
References to studies excluded from this review
-
- Aaras A, Horgen G, Bjorset HH, Ro O, Thoresen M. Musculoskeletal, visual and psychosocial stress in VDU operators before and after multidisciplinary ergonomic interventions. Applied Ergonomics 1998;29(5):335‐54. [MEDLINE: ] - PubMed
-
- Cook C, Burgess‐Limerick R. The effect of forearm support on musculoskeletal discomfort during call centre work. Applied Ergonomics 2004;35(4):337‐42. [MEDLINE: ] - PubMed
-
- Earle‐Richardson G, Jenkins PL, Strogatz D, Bell EM, Sorensen JA, May JJ. Orchard evaluation of ergonomically modified apple bucket. Journal of Agromedicine 2006;11(3‐4):95‐105. - PubMed
-
- Faucett J, Garry M, Nadler D, Ettare D. A test of two training interventions to prevent work‐related musculoskeletal disorders of the upper extremity. Applied Ergonomics 2002;33(4):337‐47. - PubMed
-
- Faucett J, Meyers J, Miles J, Janowitz I, Fathallah F. Rest break interventions in stoop labor tasks. Applied Ergonomics 2007;38(2):219‐26. - PubMed
References to ongoing studies
Additional references
-
- Bernard B, Sauter S, Fine L, Petersen M, Hales T. Job task and psychosocial risk factors for work‐related musculoskeletal disorders among newspaper employees. Scandinavian Journal of Work, Environment & Health 1994;20(6):417‐26. [PUBMED: 7701287] - PubMed
-
- Bernard BP, editor. Musculoskeletal Disorders and Workplace Factors: A Critical Review of Epidemiologic Evidence for Work‐Related Musculoskeletal Disorders of the Neck, Upper‐Extremity and Low Back. DHHS (NIOSH) Publication No. 97‐141. Cincinnati, OH: US Department of Health and Human Services, 1997.
-
- Bonfiglioli R, Mattioli S, Spagnolo MR, Violante FS. Course of symptoms and median nerve conduction values in workers performing repetitive jobs at risk for carpal tunnel syndrome. Occupational Medicine 2006;56(2):115‐21. [MEDLINE: ] - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical