

The pancreas cancer microenvironment
- PMID: 22896693
- PMCID: PMC3442232
- DOI: 10.1158/1078-0432.CCR-11-3114
The pancreas cancer microenvironment
Abstract
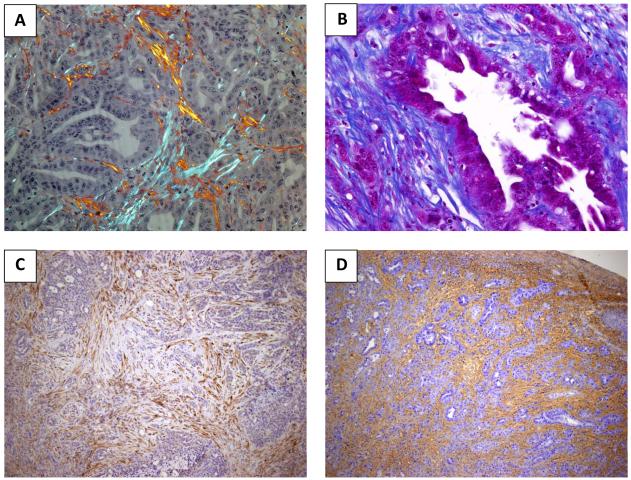
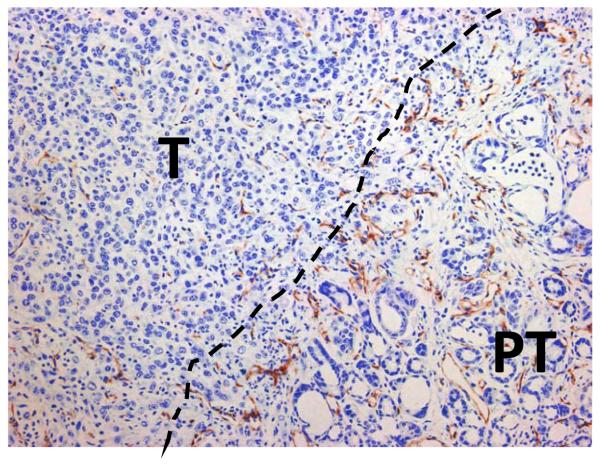
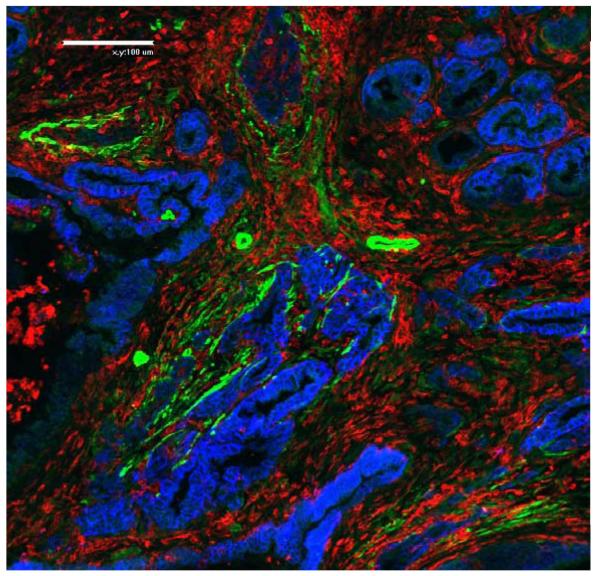
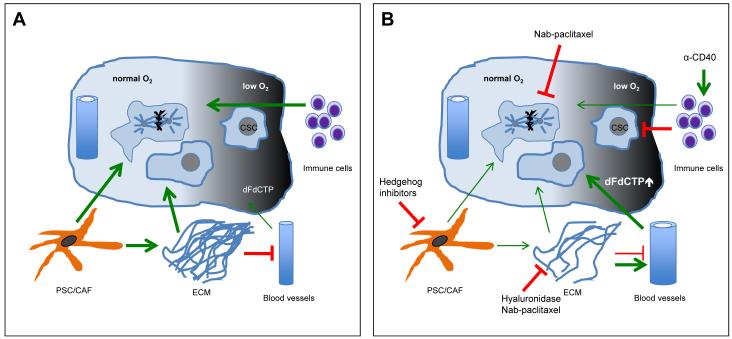
Pancreatic ductal adenocarcinoma (PDA) is a common and lethal malignancy resulting in more than 250,000 deaths per year worldwide. Despite extensive efforts, cytotoxic and targeted therapies have provided only limited efficacy for patients with PDA to date. One contributing factor to the failure of systemic therapies may be the abundant tumor stromal content that is the characteristic of PDA. The PDA stroma, aptly termed the tumor microenvironment, occupies the majority of the tumor mass, and consists of a dynamic assortment of extracellular matrix components and nonneoplastic cells including fibroblastic, vascular, and immune cells. Recent work has revealed that the PDA stroma supports tumor growth and promotes metastasis and simultaneously serves as a physical barrier to drug delivery. Accordingly, methods that alter stromal composition or function, for instance interference with the vasculature via Notch/Hedgehog pathway inhibition or relief of vascular compression by hyaluronidase, are under active investigation. Here, we will review our current understanding of the PDA tumor microenvironment, and highlight opportunities for further exploration that may benefit patients.
Figures
References
-
- Hidalgo M. Pancreatic cancer. N Engl J Med. 2010 Apr 29;362(17):1605–17. - PubMed
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J Clin. 2012 Jan-Feb;62(1):10–29. - PubMed
-
- Neoptolemos JP. Adjuvant treatment of pancreatic cancer. Eur J Cancer. 2011 Sep;47(Suppl 3):S378–80. - PubMed
-
- Yauch RL, Settleman J. Recent advances in pathway-targeted cancer drug therapies emerging from cancer genome analysis. Curr Opin Genet Dev. 2012 Feb 7; - PubMed
-
- Burris HA, 3rd, Moore MJ, Andersen J, Green MR, Rothenberg ML, Modiano MR, et al. Improvements in survival and clinical benefit with gemcitabine as first-line therapy for patients with advanced pancreas cancer: a randomized trial. J Clin Oncol. 1997 Jun;15(6):2403–13. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
