

Comparison of ultrasonography with Doppler and MRI for assessment of disease activity in juvenile idiopathic arthritis: a pilot study
- PMID: 22897976
- PMCID: PMC3608365
- DOI: 10.1186/1546-0096-10-23
Comparison of ultrasonography with Doppler and MRI for assessment of disease activity in juvenile idiopathic arthritis: a pilot study
Abstract
Background: In juvenile idiopathic arthritis (JIA), the trend towards early therapeutic intervention and the development of new highly effective treatments have increased the need for sensitive and specific imaging. Numerous studies have demonstrated the important role of MRI and US in adult rheumatology. However, investigations of imaging in JIA are rare, and no previous study has been comparing MRI with Doppler ultrasonography (US) for assessment of arthritis. The aim of the present study was to compare the two imaging methods regarding their usefulness for evaluating disease activity in JIA, and to compare the results with those obtained in healthy controls.
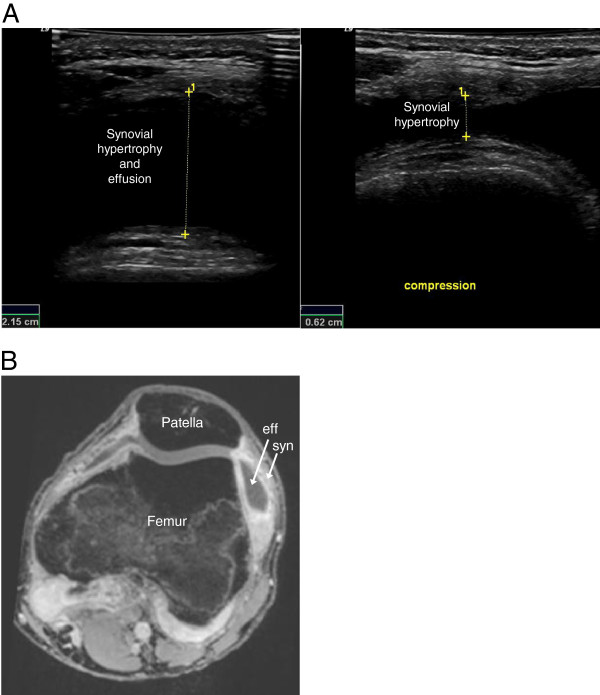
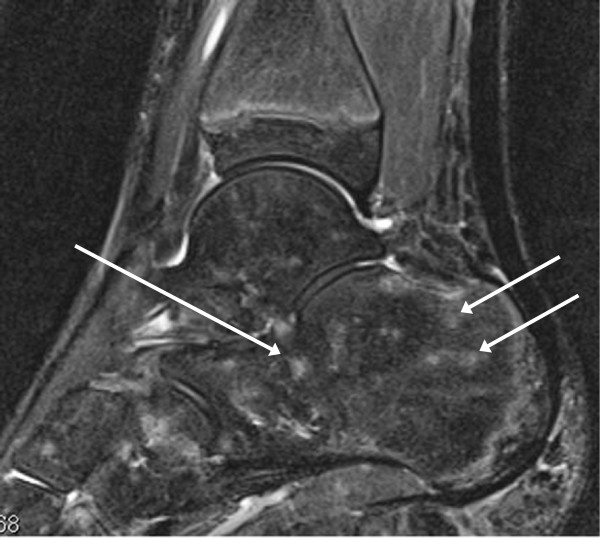
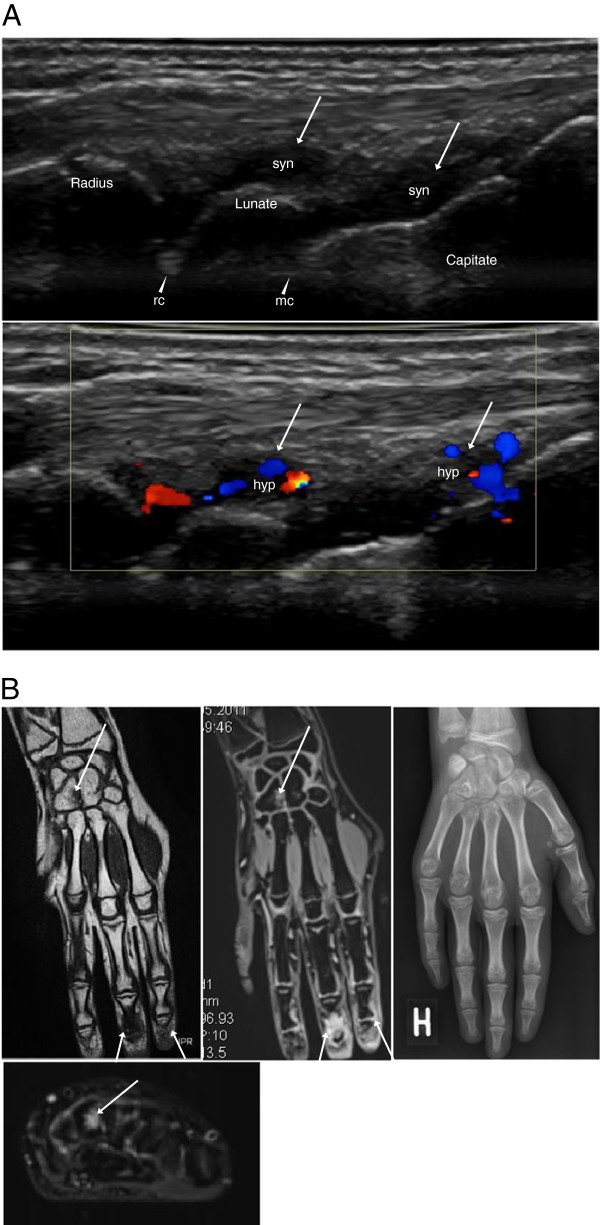
Methods: In 10 JIA patients (median age 14 years, range 11-18), 11 joints (six wrists, three knees, two ankles) with arthritis were assessed by color Doppler US and MRI. The same imaging modalities were used to evaluate eight joints (three wrists, three knees, two ankles) in six healthy age- and sex-matched controls. The US examinations of both the patients and controls were compared with the MRI findings.
Results: In 10 JIA patients, US detected synovial hypertrophy in 22 areas of 11 joints, 86% of which had synovial hyperemia, and MRI revealed synovitis in 36 areas of the same 11 joints. Erosions were identified by US in two areas of two joints and by MRI in six areas of four joints. Effusion was shown by US in nine areas of six joints and by MRI in 17 areas of five joints. MRI detected juxta-articular bone marrow edema in 16 areas of eight joints.
Conclusions: The results of this pilot study indicate that both MRI and US provide valuable imaging information on disease activity in JIA. Importantly, the two techniques seem to complement each other and give partly different information. Although MRI is considered to be the reference standard for advanced imaging in adult rheumatology, US seems to provide useful imaging information that could make it an option in daily clinical practice, in JIA as well as in adult rheumatology. However, the current work represents a pilot study, and thus our results need to be confirmed in a larger prospective clinical investigation.
Figures


References
-
- Filippou G, Cantarini L, Bertoldi I, Picerno V, Frediani B, Galeazzi M. Ultrasonography vs. clinical examination in children with suspected arthritis. Does it make sense to use poliarticular ultrasonographic screening? Clin Exp Rheumatol. 2011;29:345–350. - PubMed
-
- Guzman J, Burgos-Vargas R, Duarte-Salazar C, Gomez-Mora P. Reliability of the articular examination in children with juvenile rheumatoid arthritis: interobserver agreement and sources of disagreement. J Rheumatol. 1995;22:2331–2336. - PubMed
LinkOut - more resources
Full Text Sources
