

JAK2V617F homozygosity arises commonly and recurrently in PV and ET, but PV is characterized by expansion of a dominant homozygous subclone
- PMID: 22898600
- PMCID: PMC3672970
- DOI: 10.1182/blood-2012-05-431791
JAK2V617F homozygosity arises commonly and recurrently in PV and ET, but PV is characterized by expansion of a dominant homozygous subclone
Abstract
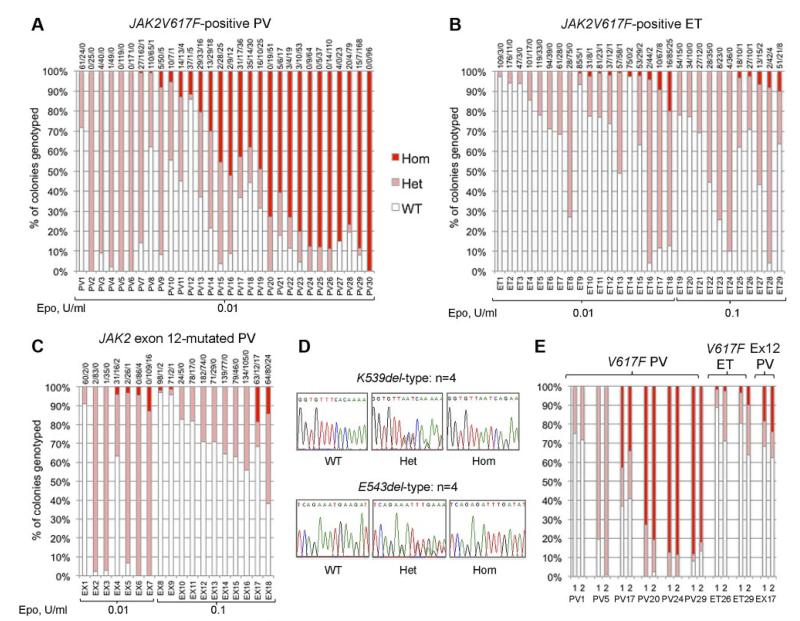
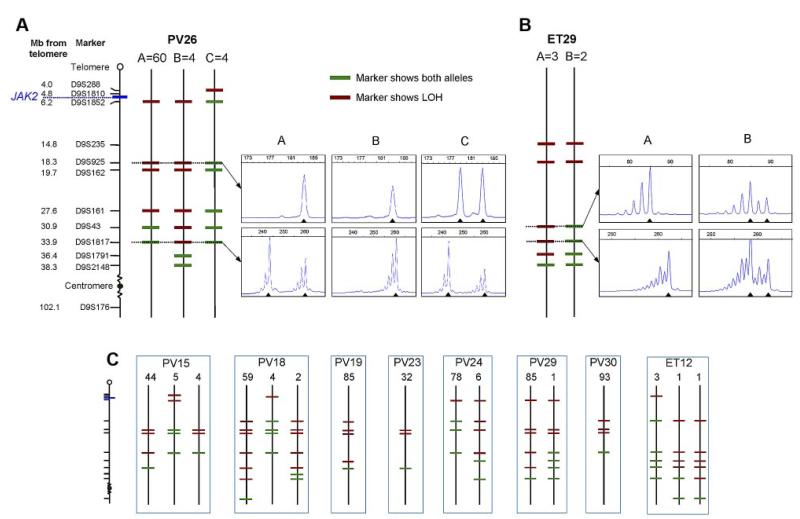
Subclones homozygous for JAK2V617F are more common in polycythemia vera (PV) than essential thrombocythemia (ET), but their prevalence and significance remain unclear. The JAK2 mutation status of 6495 BFU-E, grown in low erythropoietin conditions, was determined in 77 patients with PV or ET. Homozygous-mutant colonies were common in patients with JAK2V617F-positive PV and were surprisingly prevalent in JAK2V617F-positive ET and JAK2 exon 12-mutated PV. Using microsatellite PCR to map loss-of-heterozygosity breakpoints within individual colonies, we demonstrate that recurrent acquisition of JAK2V617F homozygosity occurs frequently in both PV and ET. PV was distinguished from ET by expansion of a dominant homozygous subclone, the selective advantage of which is likely to reflect additional genetic or epigenetic lesions. Our results suggest a model in which development of a dominant JAK2V617F-homzygous subclone drives erythrocytosis in many PV patients, with alternative mechanisms operating in those with small or undetectable homozygous-mutant clones.
Figures
References
-
- Baxter EJ, Scott LM, Campbell PJ, et al. Acquired mutation of the tyrosine kinase JAK2 in human myeloproliferative disorders. Lancet. 2005;365(9464):1054–1061. - PubMed
-
- Levine RL, Wadleigh M, Cools J, et al. Activating mutation in the tyrosine kinase JAK2 in polycythemia vera, essential thrombocythemia, and myeloid metaplasia with myelofibrosis. Cancer Cell. 2005;7(4):387–397. - PubMed
-
- James C, Ugo V, Le Couedic JP, et al. A unique clonal JAK2 mutation leading to constitutive signalling causes polycythaemia vera. Nature. 2005;434(7037):1144–1148. - PubMed
-
- Kralovics R, Passamonti F, Buser AS, et al. A gain-of-function mutation of JAK2 in myeloproliferative disorders. N Engl J Med. 2005;352(17):1779–1790. - PubMed
-
- Vannucchi AM, Antonioli E, Guglielmelli P, et al. Clinical profile of homozygous JAK2 617V>F mutation in patients with polycythemia vera or essential thrombocythemia. Blood. 2007;110(3):840–846. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
