

Imatinib after induction for treatment of children and adolescents with Philadelphia-chromosome-positive acute lymphoblastic leukaemia (EsPhALL): a randomised, open-label, intergroup study
- PMID: 22898679
- PMCID: PMC3431502
- DOI: 10.1016/S1470-2045(12)70377-7
Imatinib after induction for treatment of children and adolescents with Philadelphia-chromosome-positive acute lymphoblastic leukaemia (EsPhALL): a randomised, open-label, intergroup study
Abstract
Background: Trials of imatinib have provided evidence of activity in adults with Philadelphia-chromosome-positive acute lymphoblastic leukaemia (ALL), but the drug's role when given with multidrug chemotherapy to children is unknown. This study assesses the safety and efficacy of oral imatinib in association with a Berlin-Frankfurt-Munster intensive chemotherapy regimen and allogeneic stem-cell transplantation for paediatric patients with Philadelphia-chromosome-positive ALL.
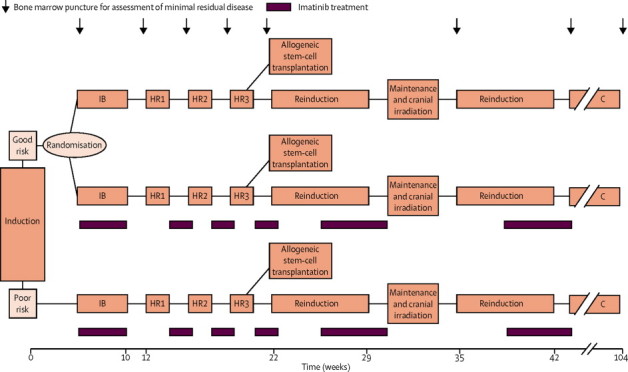
Methods: Patients aged 1-18 years recruited to national trials of front-line treatment for ALL were eligible if they had t(9;22)(q34;q11). Patients with abnormal renal or hepatic function, or an active systemic infection, were ineligible. Patients were enrolled by ten study groups between 2004 and 2009, and were classified as good risk or poor risk according to early response to induction treatment. Good-risk patients were randomly assigned by a web-based system with permuted blocks (size four) to receive post-induction imatinib with chemotherapy or chemotherapy only in a 1:1 ratio, while all poor-risk patients received post-induction imatinib with chemotherapy. Patients were stratified by study group. The chemotherapy regimen was modelled on a Berlin-Frankfurt-Munster high-risk backbone; all received four post-induction blocks of chemotherapy after which they became eligible for stem-cell transplantation. The primary endpoints were disease-free survival at 4 years in the good-risk group and event-free survival at 4 years in the poor-risk group, analysed by intention to treat and a secondary analysis of patients as treated. The trial is registered with EudraCT (2004-001647-30) and ClinicalTrials.gov, number NCT00287105.
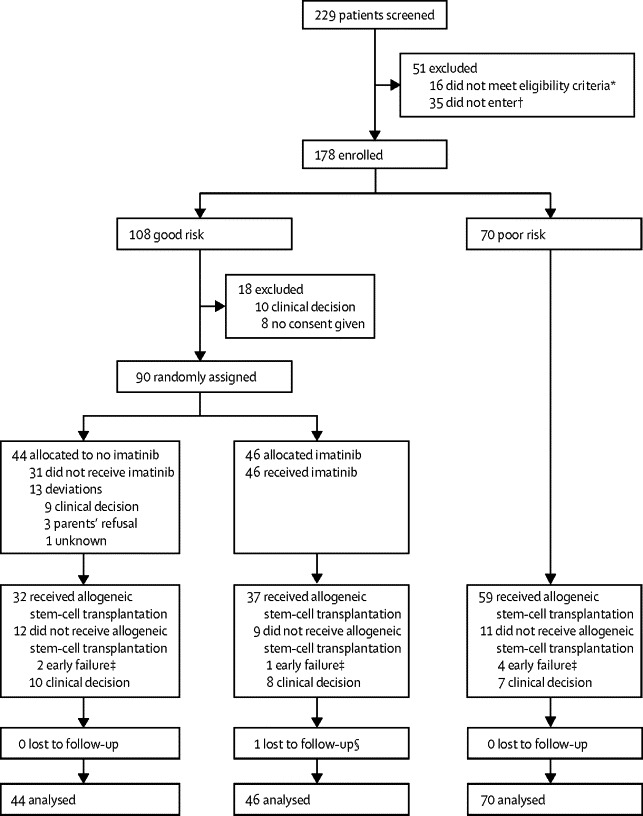
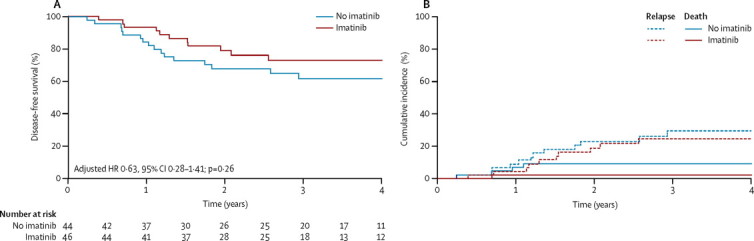
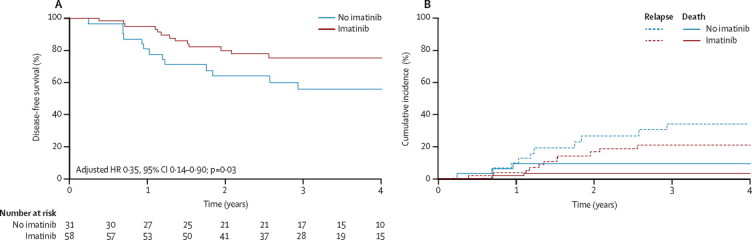
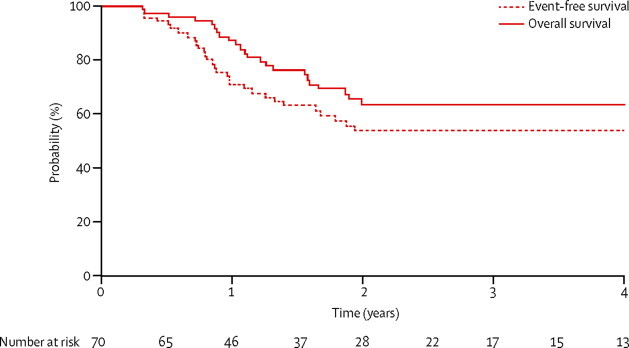
Findings: Between Jan 1, 2004, and Dec 31, 2009, we screened 229 patients and enrolled 178: 108 were good risk and 70 poor risk. 46 good-risk patients were assigned to receive imatinib and 44 to receive no imatinib. Median follow-up was 3·1 years (IQR 2·0-4·6). 4-year disease-free survival was 72·9% (95% CI 56·1-84·1) in the good-risk, imatinib group versus 61·7% (45·0-74·7) in the good-risk, no imatinib group (p=0·24). The hazard ratio (HR) for failure, adjusted for minimal residual disease, was 0·63 (0·28-1·41; p=0·26). The as-treated analysis showed 4-year disease-free survival was 75·2% (61·0-84·9) for good-risk patients receiving imatinib and 55·9% (36·1-71·7) for those who did not receive imatinib (p=0·06). 4-year event-free survival for poor-risk patients was 53·5% (40·4-65·0). Serious adverse events were much the same in the good-risk groups, with infections caused by myelosuppression the most common. 16 patients in the good-risk imatinib group versus ten in the good-risk, no imatinib group (p=0·64), and 24 in the poor-risk group, had a serious adverse event.
Interpretation: Our results suggests that imatinib in conjunction with intensive chemotherapy is well tolerated and might be beneficial for treatment of children with Philadelphia-chromosome-positive ALL.
Funding: Projet Hospitalier de Recherche Clinique-Cancer (France), Fondazione Tettamanti-De Marchi and Associazione Italiana per la Ricerca sul Cancro (Italy), Novartis Germany, Cancer Research UK, Leukaemia Lymphoma Research, and Central Manchester University Hospitals Foundation Trust.
Copyright © 2012 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Childhood Philadelphia-chromosome-positive B-lymphoblastic leukaemia.Lancet Oncol. 2012 Sep;13(9):860-2. doi: 10.1016/S1470-2045(12)70382-0. Lancet Oncol. 2012. PMID: 22935232 No abstract available.
References
-
- Aricò M, Valsecchi MG, Camitta B. Outcome of treatment in children with Philadelphia chromosome-positive acute lymphoblastic leukemia. N Engl J Med. 2000;342:998–1006. - PubMed
-
- Pui CH, Evans WE. Treatment of acute lymphoblastic leukemia. N Engl J Med. 2006;354:166–178. - PubMed
-
- Schindler T, Bornmann W, Pellicena P, Miller WT, Clarkson B, Kuriyan J. Structural mechanism for STI-571 inhibition of abelson tyrosine kinase. Science. 2000;289:1938–1942. - PubMed
-
- Heinrich MC, Blanke CD, Druker BJ, Corless CL. Inhibition of KIT tyrosine kinase activity: a novel molecular approach to the treatment of KIT–positive malignancies. J Clin Oncol. 2002;20:1692–1703. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
