

3-T MR-guided brachytherapy for gynecologic malignancies
- PMID: 22898699
- PMCID: PMC3468320
- DOI: 10.1016/j.mri.2012.06.003
3-T MR-guided brachytherapy for gynecologic malignancies
Abstract
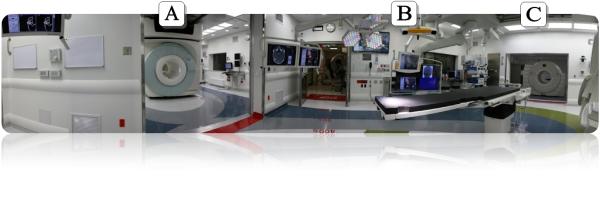
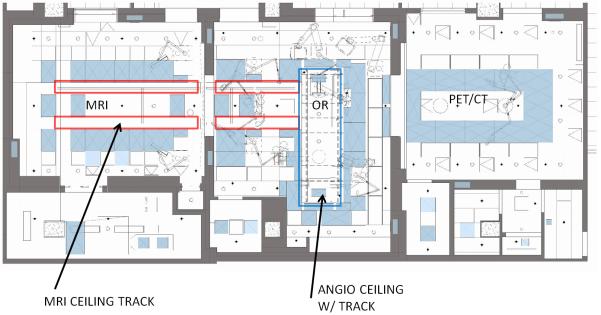
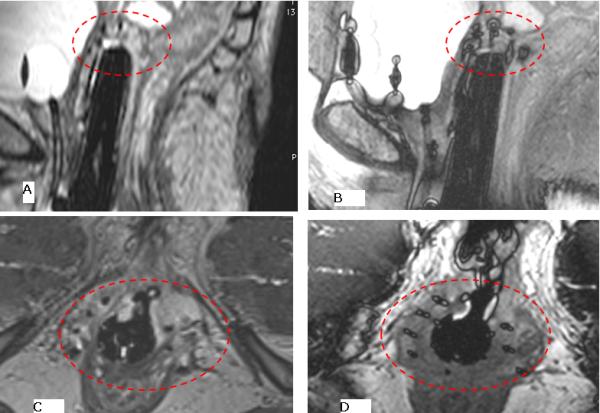
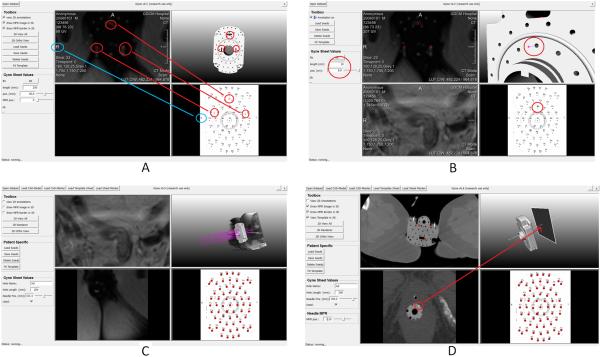
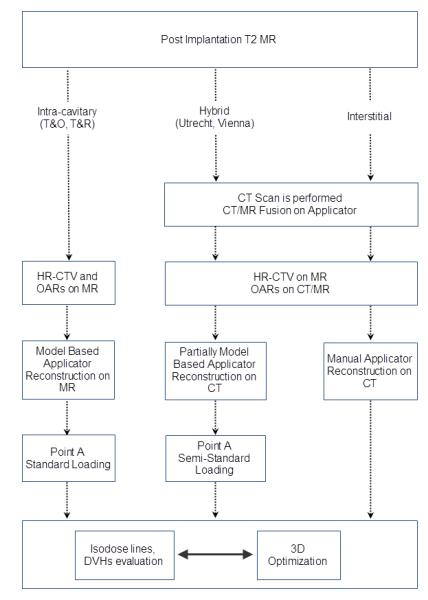
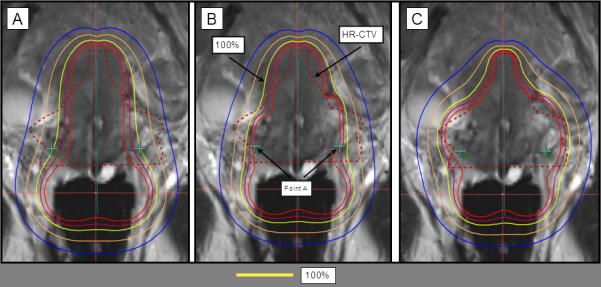
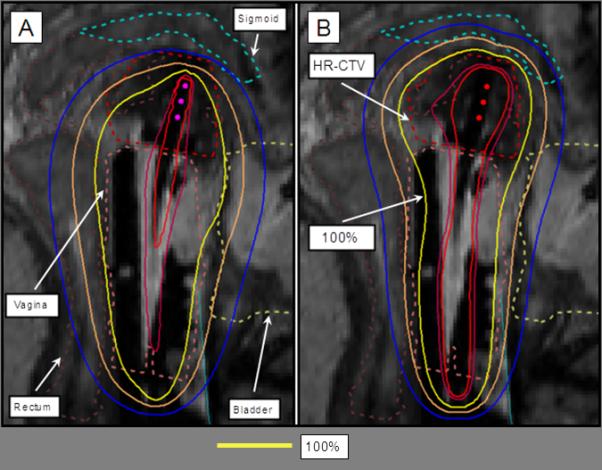
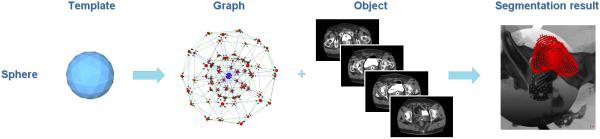
Gynecologic malignancies are a leading cause of death in women worldwide. Standard treatment for many primary and recurrent gynecologic cancer cases includes external-beam radiation followed by brachytherapy. Magnetic resonance (MR) imaging is beneficial in diagnostic evaluation, in mapping the tumor location to tailor radiation dose and in monitoring the tumor response to treatment. Initial studies of MR guidance in gynecologic brachytherapy demonstrate the ability to optimize tumor coverage and reduce radiation dose to normal tissues, resulting in improved outcomes for patients. In this article, we describe a methodology to aid applicator placement and treatment planning for 3 Tesla (3-T) MR-guided brachytherapy that was developed specifically for gynecologic cancers. This methodology has been used in 18 cases from September 2011 to May 2012 in the Advanced Multimodality Image Guided Operating (AMIGO) suite at Brigham and Women's Hospital. AMIGO comprises state-of-the-art tools for MR imaging, image analysis and treatment planning. An MR sequence using three-dimensional (3D)-balanced steady-state free precession in a 3-T MR scanner was identified as the best sequence for catheter identification with ballooning artifact at the tip. 3D treatment planning was performed using MR images. Items in development include software designed to support virtual needle trajectory planning that uses probabilistic bias correction, graph-based segmentation and image registration algorithms. The results demonstrate that 3-T MR image guidance has a role in gynecologic brachytherapy. These novel developments have the potential to improve targeted treatment to the tumor while sparing the normal tissues.
Copyright © 2012 Elsevier Inc. All rights reserved.
Figures

References
-
- Cancer Facts & Figures 2012. [ http://www.cancer.org/Research/CancerFactsFigures/CancerFactsFigures/can...]
-
- Viswanathan AN, Thomadsen B. American Brachytherapy Society consensus guidelines for locally advanced carcinoma of the cervix. Part I: General principles. Brachytherapy. 2012;11(1):33–46. - PubMed
-
- Viswanathan AN, Kirisits C, Erickson B, Pötter R. Gynecologic Radiation Therapy: Novel Approaches to Image-Guidance and Management. Springer; Berlin; London: 2011.
-
- Viswanathan AN, Moughan J, Small W, Jr., Levenback C, Iyer R, Hymes S, Dicker AP, Miller B, Erickson B, Gaffney DK. The Quality of Cervical Cancer Brachytherapy Implantation and the Impact on Local Recurrence and Disease-Free Survival in Radiation Therapy Oncology Group Prospective Trials 0116 and 0128. Int J Gynecol Cancer. 2012;22(1):123–131. - PMC - PubMed
-
- Hricak H, Gatsonis C, Coakley FV, Snyder B, Reinhold C, Schwartz LH, Woodward PJ, Pannu HK, Amendola M, Mitchell DG. Early invasive cervical cancer: CT and MR imaging in preoperative evaluation - ACRIN/GOG comparative study of diagnostic performance and interobserver variability. Radiology. 2007;245(2):491–498. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
