

Effects of neoadjuvant intraperitoneal/systemic chemotherapy (bidirectional chemotherapy) for the treatment of patients with peritoneal metastasis from gastric cancer
- PMID: 22900159
- PMCID: PMC3415092
- DOI: 10.1155/2012/148420
Effects of neoadjuvant intraperitoneal/systemic chemotherapy (bidirectional chemotherapy) for the treatment of patients with peritoneal metastasis from gastric cancer
Abstract
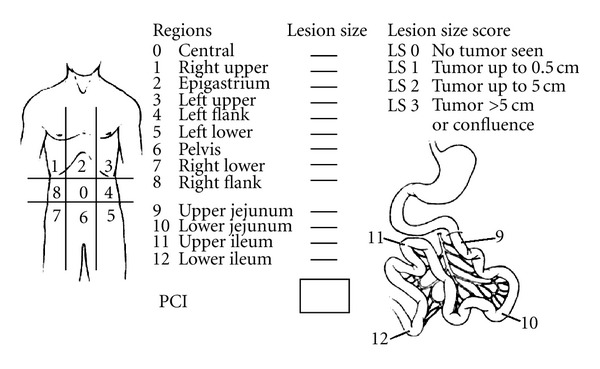
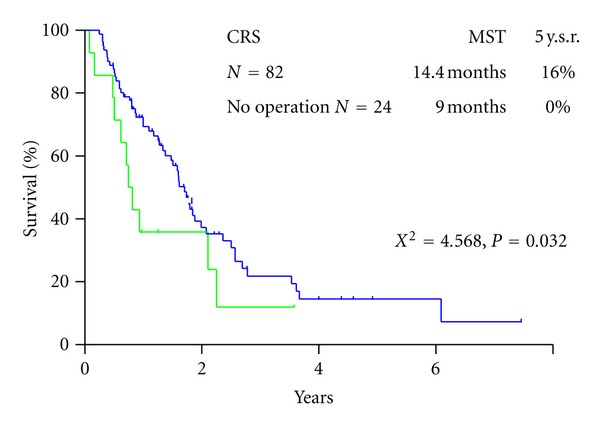
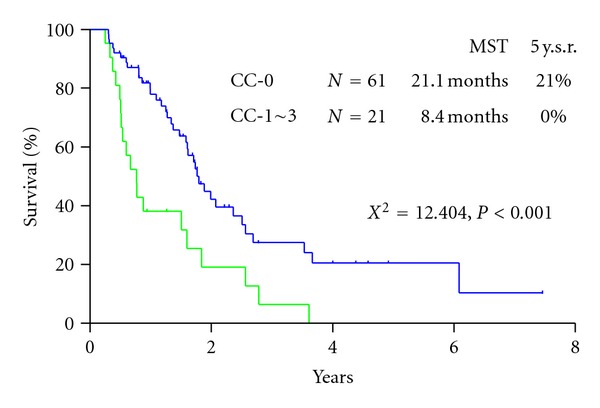
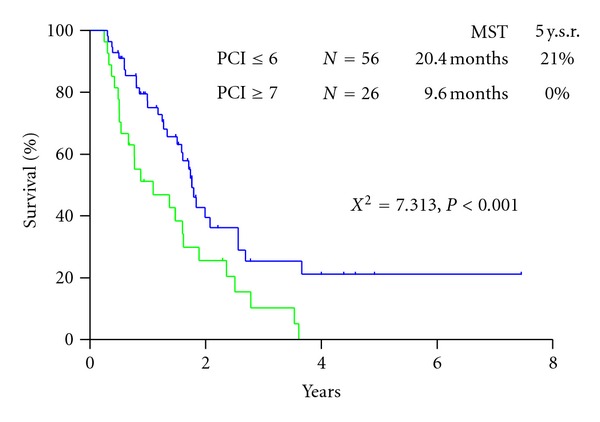
Novel multidisciplinary treatment combined with neoadjuvant intraperitoneal-systemic chemotherapy protocol (NIPS) and peritonectomy was developed. Ninety-six patients were enrolled. Peritoneal wash cytology was performed before and after NIPS through a port system. Patients were treated with 60 mg/m(2) of oral S-1 for 21 days, followed by a 1-week rest. On days 1, 8, and 15, 30 mg/m(2) of Taxotere and 30 mg/m(2) of cisplatin with 500 mL of saline were introduced through the port. NIPS is done 2 cycles before surgery. Three weeks after NIPS, 82 patients were eligible to intend cytoreductive surgery (CRS) by gastrectomy + D2 dissection + periotnectomy to achieve complete cytoreduction. Sixty-eight patients showed positice cytology before NIPS, and the positive cytology results became negative in 47 (69%) patients after NIPS. Complete pathologic response on PC after NIPS was experienced in 30 (36.8%) patients. Stage migration was experienced in 12 patients (14.6%). Complete cytoreduction was achieved in 58 patients (70.7%). By the multivariate analysis, complete cytoreduction and pathologic response became a significantly good survival. However the high morbidity and mortality, stringent patient selection is important. The best indications of the therapy are patients with good pathologic response and PCI ≤ 6, which are supposed to be removed completely by peritonectomy.
Figures
References
-
- Sadeghi B, Arvieux C, Glehen O, et al. Peritoneal carcinomatosis from non-gynecologic malignancies: results of the EVOCAPE 1 multicentric prospective study. Cancer. 2000;88(2):358–363. - PubMed
-
- Preusser P, Wilke H, Achterrath W, et al. Phase II study with the combination etoposide, doxorubicin, and cisplatin in advanced measurable gastric cancer. Journal of Clinical Oncology. 1989;7(9):1310–1317. - PubMed
-
- Ajani JA, Ota DM, Jessup JM, et al. Resectable gastric carcinoma: an evaluation of preoperative and postoperative chemotherapy. Cancer. 1991;68(7):1501–1506. - PubMed
-
- Yonemura Y, Bandou E, Kinoshita K, et al. Effective therapy for peritoneal dissemination in gastric cancer. Surgical Oncology Clinics of North America. 2003;12(3):635–648. - PubMed
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
