

Reduced soluble receptor for advanced glycation end-products (sRAGE) scavenger capacity precedes pre-eclampsia in Type 1 diabetes
- PMID: 22900949
- PMCID: PMC3980671
- DOI: 10.1111/j.1471-0528.2012.03463.x
Reduced soluble receptor for advanced glycation end-products (sRAGE) scavenger capacity precedes pre-eclampsia in Type 1 diabetes
Abstract
Objective: Increased advanced glycation end-products (AGEs) and their soluble receptors (sRAGE) have been implicated in the pathogenesis of pre-eclampsia (PE). However, this association has not been elucidated in pregnancies complicated by diabetes. We aimed to investigate the serum levels of these factors in pregnant women with Type 1 diabetes mellitus (T1DM), a condition associated with a four-fold increase in PE.
Design: Prospective study in women with T1DM at 12.2 ± 1.9, 21.6 ± 1.5 and 31.5 ± 1.7 weeks of gestation [mean ± standard deviation (SD); no overlap] before PE onset.
Setting: Antenatal clinics.
Population: Pregnant women with T1DM (n = 118; 26 developed PE) and healthy nondiabetic pregnant controls (n = 21).
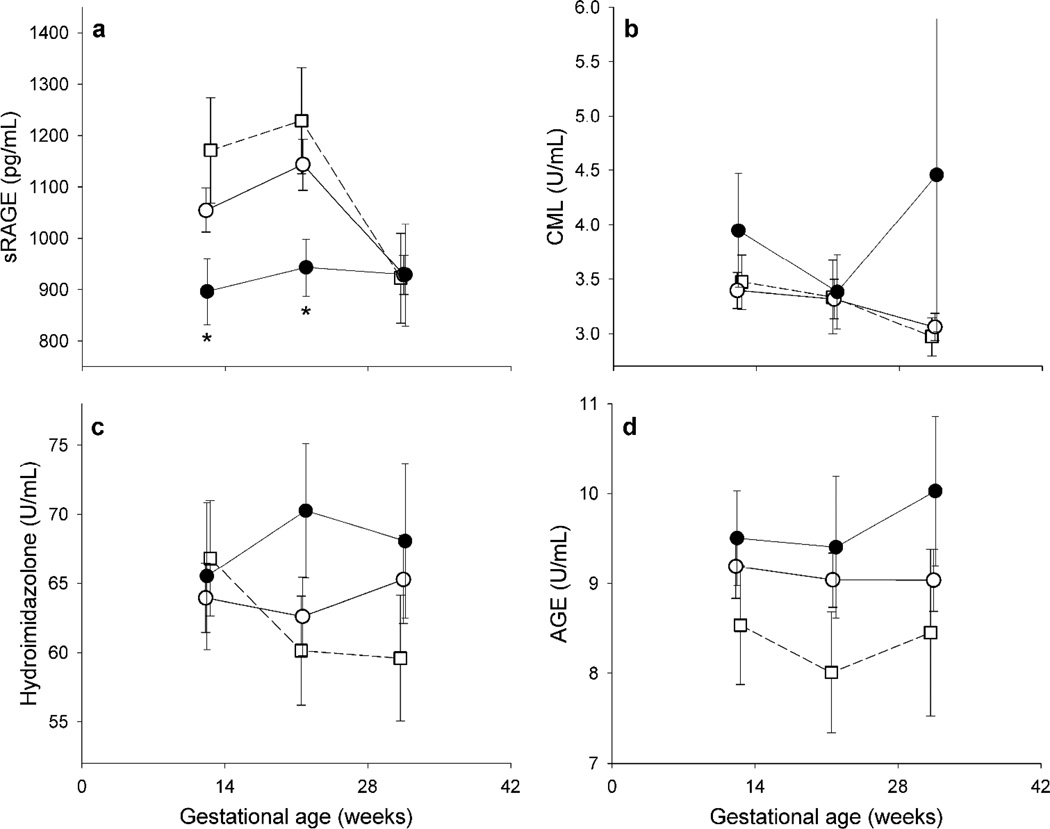
Methods: Maternal serum levels of sRAGE (total circulating pool), N(ε)-(carboxymethyl)lysine (CML), hydroimidazolone (methylglyoxal-modified proteins) and total AGEs were measured by immunoassays.
Main outcome measures: Serum sRAGE and AGEs in pregnant women with T1DM who subsequently developed PE (DM PE+) versus those who remained normotensive (DM PE-).
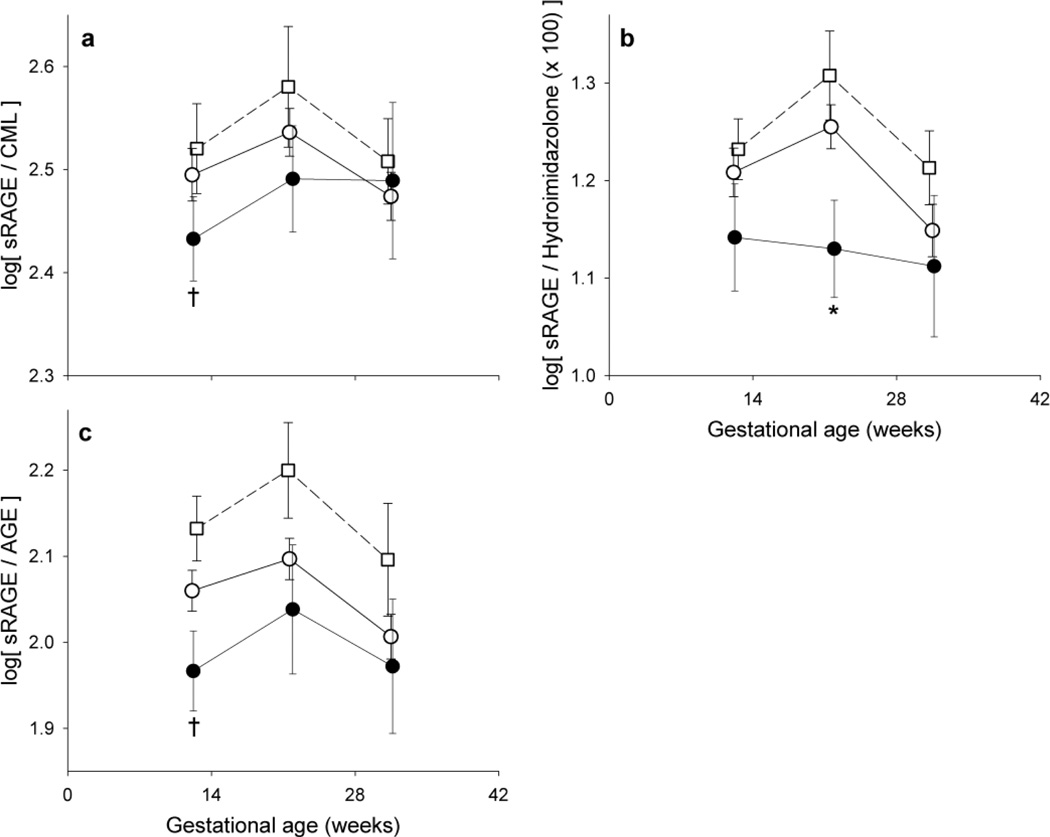
Results: In DM PE+ versus DM PE-, sRAGE was significantly lower in the first and second trimesters, prior to the clinical manifestation of PE (P < 0.05). Further, reflecting the net sRAGE scavenger capacity, sRAGE:hydroimidazolone was significantly lower in the second trimester (P < 0.05) and sRAGE:AGE and sRAGE:CML tended to be lower in the first trimester (P < 0.1) in women with T1DM who subsequently developed PE versus those who did not. These conclusions persisted after adjusting for prandial status, glycated haemoglobin (HbA1c), duration of diabetes, parity and mean arterial pressure as covariates.
Conclusions: In the early stages of pregnancy, lower circulating sRAGE levels, and the ratio of sRAGE to AGEs, may be associated with the subsequent development of PE in women with T1DM.
© 2012 The Authors BJOG An International Journal of Obstetrics and Gynaecology © 2012 RCOG.
Figures
Similar articles
-
Decrease in circulating concentrations of soluble receptors for advanced glycation end products at the time of seroconversion to autoantibody positivity in children with prediabetes.Diabetes Care. 2015 Apr;38(4):665-70. doi: 10.2337/dc14-1186. Epub 2015 Jan 8. Diabetes Care. 2015. PMID: 25573878
-
Glycation endproducts, soluble receptor for advanced glycation endproducts and cytokines in diabetic and non-diabetic pregnancies.Am J Reprod Immunol. 2009 Feb;61(2):175-82. doi: 10.1111/j.1600-0897.2008.00679.x. Am J Reprod Immunol. 2009. PMID: 19143681
-
Subclinical First Trimester Renal Abnormalities Are Associated With Preeclampsia in Normoalbuminuric Women With Type 1 Diabetes.Diabetes Care. 2018 Jan;41(1):120-127. doi: 10.2337/dc17-1635. Epub 2017 Nov 9. Diabetes Care. 2018. PMID: 29122892 Free PMC article.
-
Association between the soluble receptor for advanced glycation end products and diabetes mellitus: systematic review and meta-analysis.BMC Endocr Disord. 2024 Oct 30;24(1):232. doi: 10.1186/s12902-024-01759-2. BMC Endocr Disord. 2024. PMID: 39472884 Free PMC article.
-
Circulating Advanced Glycation End Products and Their Soluble Receptors in Relation to All-Cause and Cardiovascular Mortality: A Systematic Review and Meta-analysis of Prospective Observational Studies.Adv Nutr. 2021 Dec 1;12(6):2157-2171. doi: 10.1093/advances/nmab072. Adv Nutr. 2021. PMID: 34139010 Free PMC article.
Cited by
-
Arginine vasopressin infusion is sufficient to model clinical features of preeclampsia in mice.JCI Insight. 2018 Oct 4;3(19):e99403. doi: 10.1172/jci.insight.99403. JCI Insight. 2018. PMID: 30282823 Free PMC article.
-
Plasma AGE and Oxidation Products, Renal Function, and Preeclampsia in Pregnant Women with Type 1 Diabetes: A Prospective Observational Study.J Diabetes Res. 2023 Aug 10;2023:8537693. doi: 10.1155/2023/8537693. eCollection 2023. J Diabetes Res. 2023. PMID: 37601831 Free PMC article.
-
Glycation of LDL: AGEs, impact on lipoprotein function, and involvement in atherosclerosis.Front Cardiovasc Med. 2023 Jan 24;10:1094188. doi: 10.3389/fcvm.2023.1094188. eCollection 2023. Front Cardiovasc Med. 2023. PMID: 36760567 Free PMC article. Review.
-
Soluble RAGE and atherosclerosis in youth with type 1 diabetes: a 5-year follow-up study.Cardiovasc Diabetol. 2015 Sep 25;14:126. doi: 10.1186/s12933-015-0292-2. Cardiovasc Diabetol. 2015. PMID: 26408307 Free PMC article.
-
Circulating Levels of the Soluble Receptor for AGE (sRAGE) during Escalating Oral Glucose Dosages and Corresponding Isoglycaemic i.v. Glucose Infusions in Individuals with and without Type 2 Diabetes.Nutrients. 2020 Sep 24;12(10):2928. doi: 10.3390/nu12102928. Nutrients. 2020. PMID: 32987824 Free PMC article.
References
-
- Roberts JM, Pearson G, Cutler J, Lindheimer M. Summary of the NHLBI Working Group on Research on Hypertension During Pregnancy. Hypertension. 2003;41:437–445. - PubMed
-
- Hanson U, Persson B. Outcome of pregnancies complicated by type 1 insulin-dependent diabetes in Sweden: acute pregnancy complications, neonatal mortality and morbidity. Am J Perinatol. 1993;10:330–333. - PubMed
-
- Hsu CD, Tan HY, Hong SF, Nickless NA, Copel JA. Strategies for reducing the frequency of preeclampsia in pregnancies with insulin-dependent diabetes mellitus. Am J Perinatol. 1996;13:265–268. - PubMed
-
- Yu Y, Jenkins AJ, Nankervis AJ, Hanssen KF, Scholz H, Henriksen T, et al. Anti-angiogenic factors and pre-eclampsia in type 1 diabetic women. Diabetologia. 2009;52:160–168. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
