

Updated results of magnetic resonance imaging guided partial prostate brachytherapy for favorable risk prostate cancer: implications for focal therapy
- PMID: 22901567
- PMCID: PMC3744091
- DOI: 10.1016/j.juro.2012.06.010
Updated results of magnetic resonance imaging guided partial prostate brachytherapy for favorable risk prostate cancer: implications for focal therapy
Abstract
Purpose: We report updated results of magnetic resonance imaging guided partial prostate brachytherapy and propose a definition of biochemical failure following focal therapy.
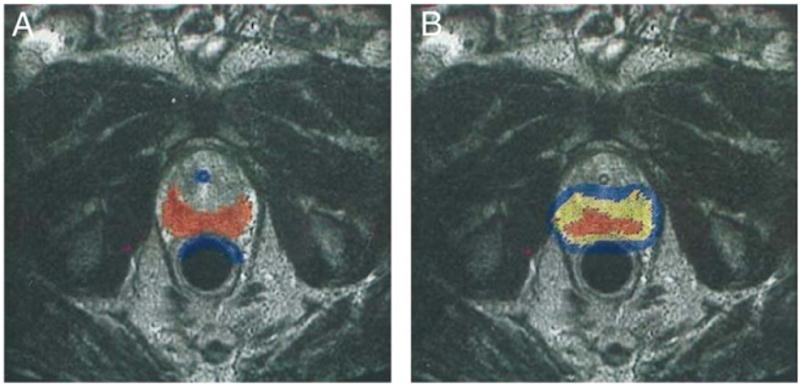
Materials and methods: From 1997 to 2007, 318 men with cT1c, prostate specific antigen less than 15 ng/ml, Gleason 3 + 4 or less prostate cancer received magnetic resonance imaging guided brachytherapy in which only the peripheral zone was targeted. To exclude benign prostate specific antigen increases due to prostatic hyperplasia, we investigated the usefulness of defining prostate specific antigen failure as nadir +2 with prostate specific antigen velocity greater than 0.75 ng/ml per year. Cox regression was used to determine the factors associated with prostate specific antigen failure.
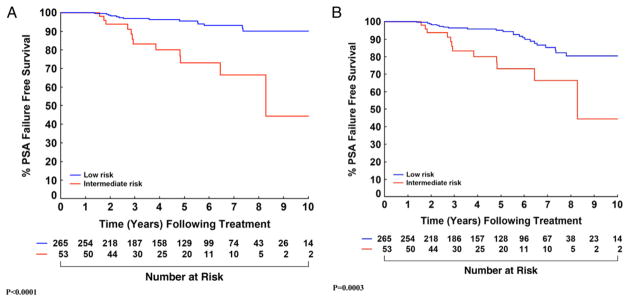
Results: Median followup was 5.1 years (maximum 12.1). While 36 patients met the nadir +2 criteria, 16 of 17 biopsy proven local recurrences were among the 26 men who also had a prostate specific antigen velocity greater than 0.75 ng/ml per year (16 of 26 vs 1 of 10, p = 0.008). Using the nadir +2 definition, prostate specific antigen failure-free survival for low risk cases at 5 and 8 years was 95.1% (91.0-97.3) and 80.4% (70.7-87.1), respectively. This rate improved to 95.6% (91.6-97.7) and 90.0% (82.6-94.3) using nadir +2 with prostate specific antigen velocity greater than 0.75 ng/ml per year. For intermediate risk cases survival was 73.0% (55.0-84.8) at 5 years and 66.4% (44.8-81.1) at 8 years (the same values as using nadir +2 with prostate specific antigen velocity greater than 0.75 ng/ml per year).
Conclusions: Requiring a prostate specific antigen velocity greater than 0.75 ng/ml per year in addition to nadir +2 appears to better predict clinical failure after therapies that target less than the whole gland. Further followup will determine whether magnetic resonance imaging guided brachytherapy targeting the peripheral zone produces comparable cancer control to whole gland treatment in men with low risk disease. However, at this time it does not appear adequate for men with even favorable intermediate risk disease.
Copyright © 2012 American Urological Association Education and Research, Inc. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Onik G, Narayan P, Vaughan D, et al. Focal “nerve-sparing” cryosurgery for treatment of primary prostate cancer: a new approach to preserving potency. Urology. 2002;60:109. - PubMed
-
- Bahn DK, Silverman P, Lee F, Sr, et al. Focal prostate cryoablation: initial results show cancer control and potency preservation. J Endourol. 2006;20:688. - PubMed
-
- Lambert EH, Bolte K, Masson P, et al. Focal cryosurgery: encouraging health outcomes for unifocal prostate cancer. Urology. 2007;69:1117. - PubMed
-
- Onik G, Vaughan D, Lotenfoe R, et al. The “male lumpectomy”: focal therapy for prostate cancer using cryoablation results in 48 patients with at least 2-year follow-up. Urol Oncol. 2008;26:500. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
