

Task shifting of antiretroviral treatment from doctors to primary-care nurses in South Africa (STRETCH): a pragmatic, parallel, cluster-randomised trial
- PMID: 22901955
- PMCID: PMC3442223
- DOI: 10.1016/S0140-6736(12)60730-2
Task shifting of antiretroviral treatment from doctors to primary-care nurses in South Africa (STRETCH): a pragmatic, parallel, cluster-randomised trial
Abstract
Background: Robust evidence of the effectiveness of task shifting of antiretroviral therapy (ART) from doctors to other health workers is scarce. We aimed to assess the effects on mortality, viral suppression, and other health outcomes and quality indicators of the Streamlining Tasks and Roles to Expand Treatment and Care for HIV (STRETCH) programme, which provides educational outreach training of nurses to initiate and represcribe ART, and to decentralise care.
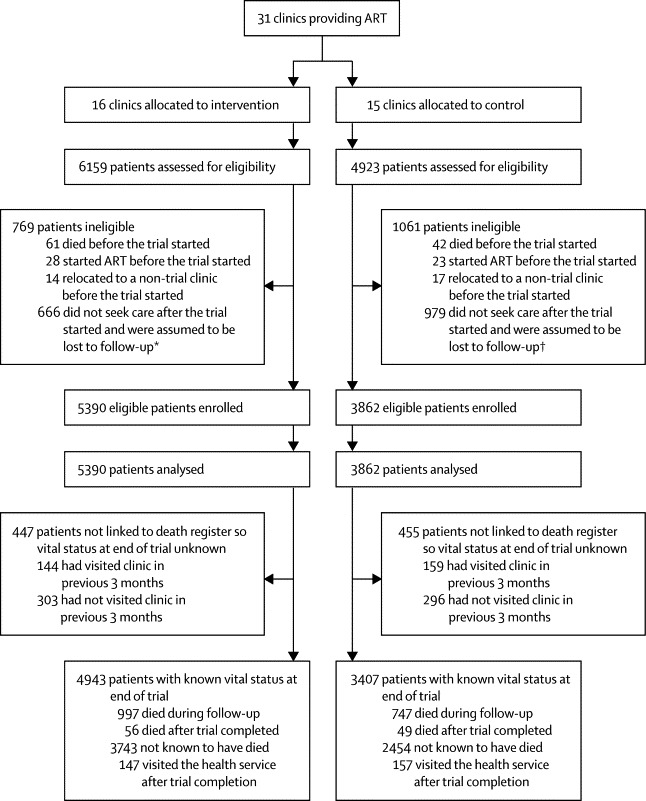
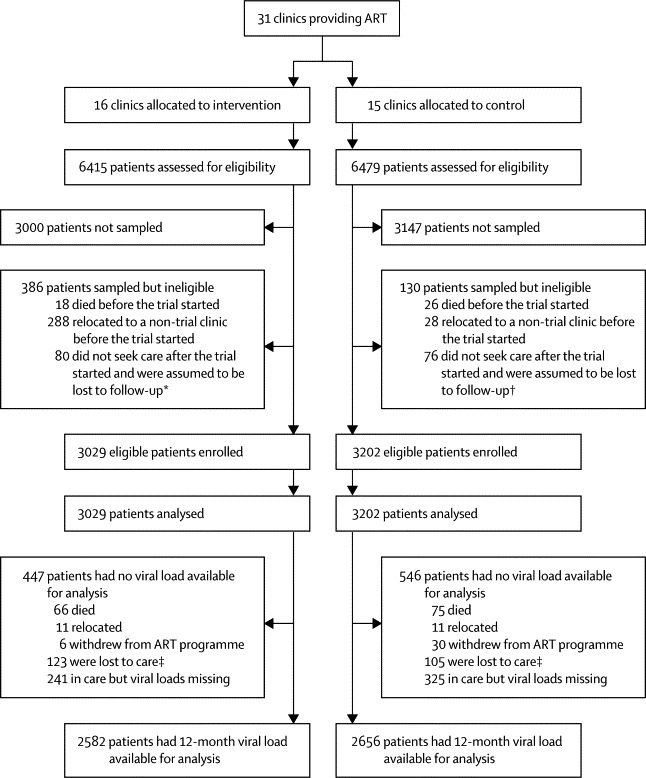
Methods: We undertook a pragmatic, parallel, cluster-randomised trial in South Africa between Jan 28, 2008, and June 30, 2010. We randomly assigned 31 primary-care ART clinics to implement the STRETCH programme (intervention group) or to continue with standard care (control group). The ratio of randomisation depended on how many clinics were in each of nine strata. Two cohorts were enrolled: eligible patients in cohort 1 were adults (aged ≥16 years) with CD4 counts of 350 cells per μL or less who were not receiving ART; those in cohort 2 were adults who had already received ART for at least 6 months and were being treated at enrolment. The primary outcome in cohort 1 was time to death (superiority analysis). The primary outcome in cohort 2 was the proportion with undetectable viral loads (<400 copies per mL) 12 months after enrolment (equivalence analysis, prespecified difference <6%). Patients and clinicians could not be masked to group assignment. The interim analysis was blind, but data analysts were not masked after the database was locked for final analysis. Analyses were done by intention to treat. This trial is registered, number ISRCTN46836853.
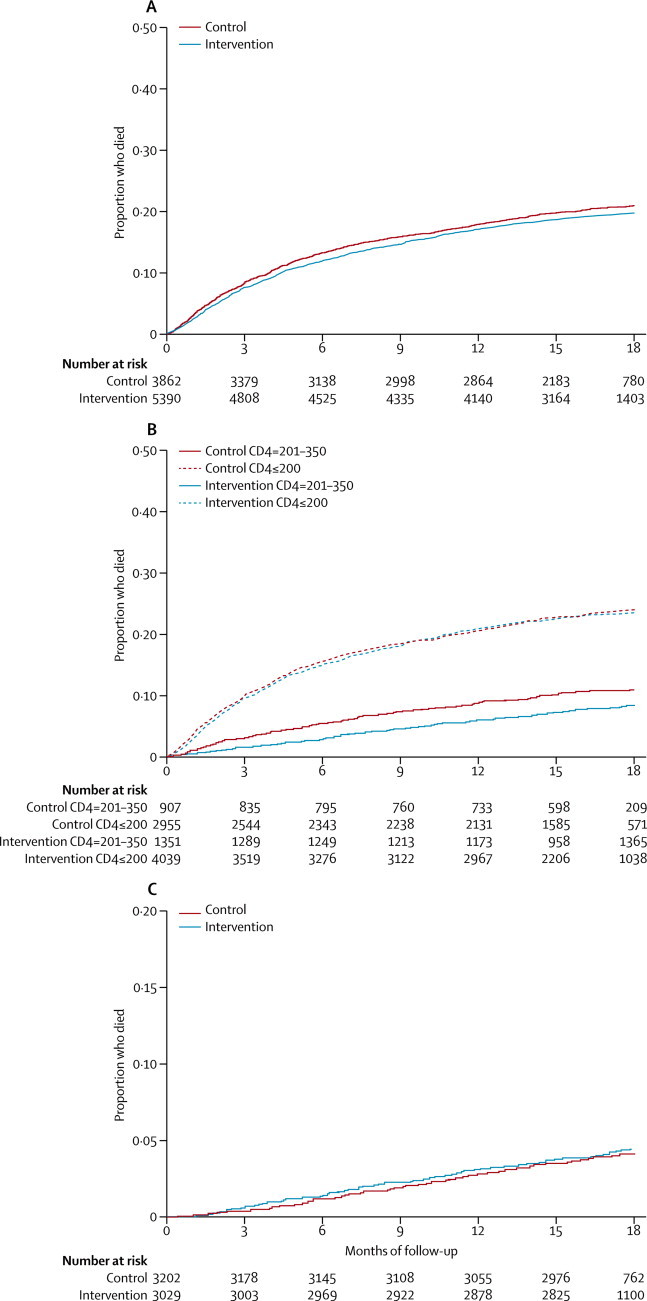
Findings: 5390 patients in cohort 1 and 3029 in cohort 2 were in the intervention group, and 3862 in cohort 1 and 3202 in cohort 2 were in the control group. Median follow-up was 16·3 months (IQR 12·2-18·0) in cohort 1 and 18·0 months (18·0-18·0) in cohort 2. In cohort 1, 997 (20%) of 4943 patients analysed in the intervention group and 747 (19%) of 3862 in the control group with known vital status at the end of the trial had died. Time to death did not differ (hazard ratio [HR] 0·94, 95% CI 0·76-1·15). In a preplanned subgroup analysis of patients with baseline CD4 counts of 201-350 cells per μL, mortality was slightly lower in the intervention group than in the control group (0·73, 0·54-1.00; p=0·052), but it did not differ between groups in patients with baseline CD4 of 200 cells per μL or less (0·94, 0·76-1·15; p=0·577). In cohort 2, viral load suppression 12 months after enrolment was equivalent in intervention (2156 [71%] of 3029 patients) and control groups (2230 [70%] of 3202; risk difference 1·1%, 95% CI -2·4 to 4·6).
Interpretation: Expansion of primary-care nurses' roles to include ART initiation and represcription can be done safely, and improve health outcomes and quality of care, but might not reduce time to ART or mortality.
Funding: UK Medical Research Council, Development Cooperation Ireland, and Canadian International Development Agency.
Copyright © 2012 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
STRETCHing delivery of HIV health services.Lancet. 2012 Sep 8;380(9845):865-7. doi: 10.1016/S0140-6736(12)60952-0. Epub 2012 Aug 15. Lancet. 2012. PMID: 22901954 No abstract available.
-
Sustainability of task-shifting for antiretroviral treatment.Lancet. 2012 Dec 1;380(9857):1907-8; author reply 1908. doi: 10.1016/S0140-6736(12)62110-2. Lancet. 2012. PMID: 23200500 Free PMC article. No abstract available.
References
-
- WHO Task shifting: global recommendations and guidelines. 2008. http://www.who.int/workforcealliance/knowledge/resources/taskshifting_gu... (accessed June 25, 2012).
-
- Fairall LR, Bachmann MO, Louwagie G. Effectiveness of antiretroviral treatment in a South African program: cohort study. Arch Intern Med. 2008;168:86–93. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
