

Preventing smoking relapse via Web-based computer-tailored feedback: a randomized controlled trial
- PMID: 22903145
- PMCID: PMC3510689
- DOI: 10.2196/jmir.2057
Preventing smoking relapse via Web-based computer-tailored feedback: a randomized controlled trial
Abstract
Background: Web-based computer-tailored approaches have the potential to be successful in supporting smoking cessation. However, the potential effects of such approaches for relapse prevention and the value of incorporating action planning strategies to effectively prevent smoking relapse have not been fully explored. The Stay Quit for You (SQ4U) study compared two Web-based computer-tailored smoking relapse prevention programs with different types of planning strategies versus a control group.
Objectives: To assess the efficacy of two Web-based computer-tailored programs in preventing smoking relapse compared with a control group. The action planning (AP) program provided tailored feedback at baseline and invited respondents to do 6 preparatory and coping planning assignments (the first 3 assignments prior to quit date and the final 3 assignments after quit date). The action planning plus (AP+) program was an extended version of the AP program that also provided tailored feedback at 11 time points after the quit attempt. Respondents in the control group only filled out questionnaires. The study also assessed possible dose-response relationships between abstinence and adherence to the programs.
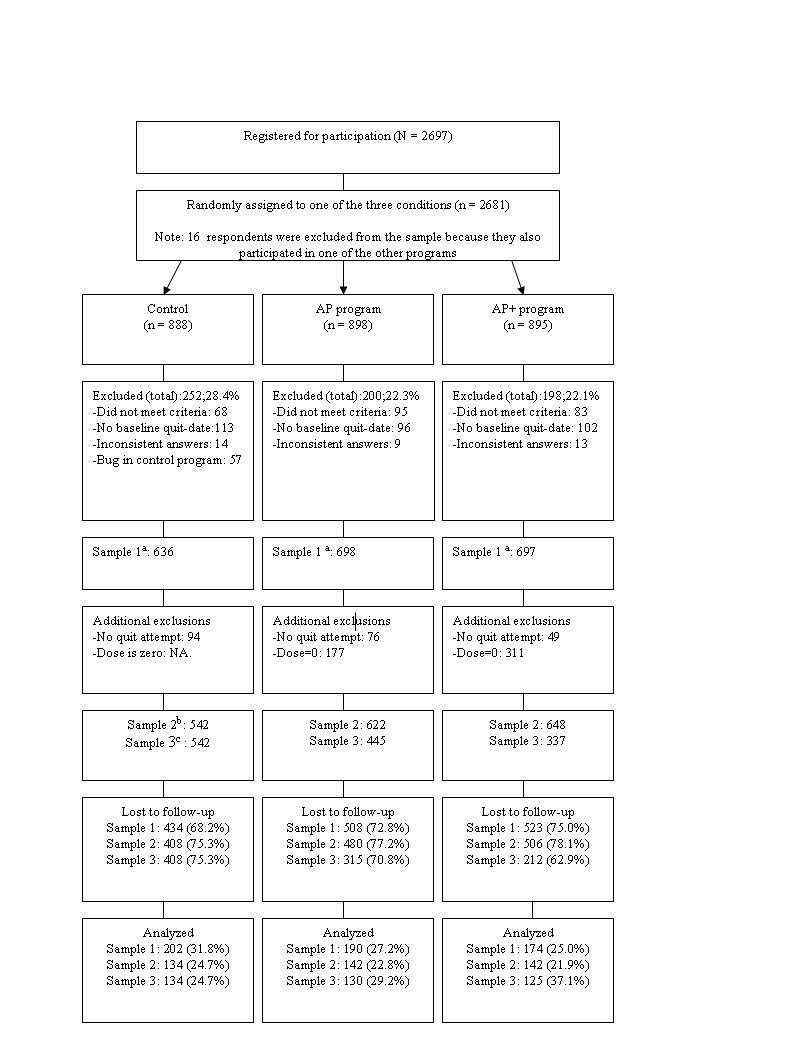
Methods: The study was a randomized controlled trial with three conditions: the control group, the AP program, and the AP+ program. Respondents were daily smokers (N = 2031), aged 18 to 65 years, who were motivated and willing to quit smoking within 1 month. The primary outcome was self-reported continued abstinence 12 months after baseline. Logistic regression analyses were conducted using three samples: (1) all respondents as randomly assigned, (2) a modified sample that excluded respondents who did not make a quit attempt in conformance with the program protocol, and (3) a minimum dose sample that also excluded respondents who did not adhere to at least one of the intervention elements. Observed case analyses and conservative analyses were conducted.
Results: In the observed case analysis of the randomized sample, abstinence rates were 22% (45/202) in the control group versus 33% (63/190) in the AP program and 31% (53/174) in the AP+ program. The AP program (odds ratio 1.95, P = .005) and the AP+ program (odds ratio 1.61, P = .049) were significantly more effective than the control condition. Abstinence rates and effects differed per sample. Finally, the results suggest a dose-response relationship between abstinence and the number of program elements completed by the respondents.
Conclusion: Despite the differences in results caused by the variation in our analysis approaches, we can conclude that Web-based computer-tailored programs combined with planning strategy assignments and feedback after the quit attempt can be effective in preventing relapse 12 months after baseline. However, adherence to the intervention seems critical for effectiveness. Finally, our results also suggest that more research is needed to assess the optimum intervention dose.
Trial registration: Dutch Trial Register: NTR1892; http://www.trialregister.nl/trialreg/admin/rctview.asp?TC=1892 (Archived by WebCite at http://www.webcitation.org/693S6uuPM).
Conflict of interest statement
None declared.
Figures
References
-
- Hughes JR, Keely J, Naud S. Shape of the relapse curve and long-term abstinence among untreated smokers. Addiction. 2004 Jan;99(1):29–38.540 - PubMed
-
- Dijkstra A, Borland R. Residual outcome expectations and relapse in ex-smokers. Health Psychol. 2003 Jul;22(4):340–6. - PubMed
-
- Kenford SL, Smith SS, Wetter DW, Jorenby DE, Fiore MC, Baker TB. Predicting relapse back to smoking: contrasting affective and physical models of dependence. J Consult Clin Psychol. 2002 Feb;70(1):216–27. - PubMed
-
- Killen JD, Fortmann SP, Kraemer HC, Varady AN, Davis L, Newman B. Interactive effects of depression symptoms, nicotine dependence, and weight change on late smoking relapse. J Consult Clin Psychol. 1996 Oct;64(5):1060–7. - PubMed
-
- Marlatt GA, Gordon JA. Relapse Prevention: Maintenance Strategies in the Treatment of Addictive Behaviors. New York, NY: Guilford Press; 1985.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
