

Cardiac imaging techniques for physicians: late enhancement
- PMID: 22903654
- PMCID: PMC3428749
- DOI: 10.1002/jmri.23605
Cardiac imaging techniques for physicians: late enhancement
Abstract
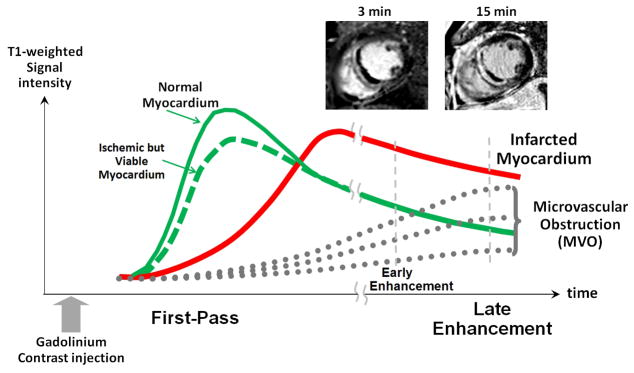
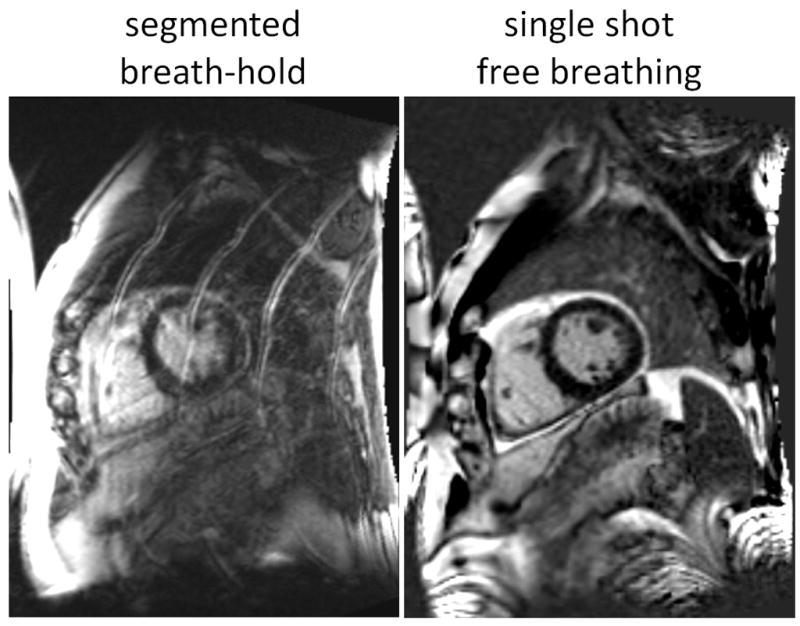
Late enhancement imaging is used to diagnose and characterize a wide range of ischemic and nonischemic cardiomyopathies, and its use has become ubiquitous in the cardiac MR exam. As the use of late enhancement imaging has matured and the span of applications has widened, the demands on image quality have grown. The characterization of subendocardial MI now includes the accurate quantification of scar size, shape, and characterization of borders which have been shown to have prognostic significance. More diverse patterns of late enhancement including patchy, mid-wall, subepicardial, or diffuse enhancement are of interest in diagnosing nonischemic cardiomyopathies. As clinicians are examining late enhancement images for more subtle indication of fibrosis, the demand for lower artifacts has increased. A range of new techniques have emerged to improve the speed and quality of late enhancement imaging including: methods for acquisition during free breathing, and fat water separated imaging for characterizing fibrofatty infiltration and reduction of artifacts related to the presence of fat. Methods for quantification of T1 and extracellular volume fraction are emerging to tackle the issue of discriminating globally diffuse fibrosis from normal healthy tissue which is challenging using conventional late enhancement methods. The aim of this review will be to describe the current state of the art and to provide a guide to various clinical protocols that are commonly used.
Published 2012 Wiley Periodicals, Inc.
Figures














References
-
- Kim RJ, Fieno DS, Parrish TB, et al. Relationship of MRI delayed contrast enhancement to irreversible injury, infarct age, and contractile function. Circulation. 1999;100:1992–2002. - PubMed
-
- Fieno DS, Kim RJ, Chen EL, Lomasney JW, Klocke FJ, Judd RM. Contrast-enhanced magnetic resonance imaging of myocardium at risk: distinction between reversible and irreversible injury throughout infarct healing. J Am Coll Cardiol. 2000;36:1985–1991. - PubMed
-
- Hunold P, Schlosser T, Vogt FM, et al. Myocardial late enhancement in contrast-enhanced cardiac MRI: distinction between infarction scar and non-infarction-related disease. Am J Roentgenol. 2005 May;184(5):1420–6. - PubMed
-
- Bohl S, Wassmuth R, Abdel-Aty H, Rudolph A, Messroghli D, Dietz R, Schulz-Menger J. Delayed enhancement cardiac magnetic resonance imaging reveals typical patterns of myocardial injury in patients with various forms of non-ischemic heart disease. Int J Cardiovasc Imaging. 2008 Aug;24(6):597–607. - PubMed
-
- Vergara GR, Marrouche NF. Tailored management of atrial fibrillation using a LGE-MRI based model: from the clinic to the electrophysiology laboratory. J Cardiovasc Electrophysiol. 2011 Apr;22(4):481–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
