

Treatment of critically ill children with kidney injury by sustained low-efficiency daily diafiltration
- PMID: 22903659
- PMCID: PMC3491203
- DOI: 10.1007/s00467-012-2254-1
Treatment of critically ill children with kidney injury by sustained low-efficiency daily diafiltration
Abstract
Background: Continuous renal replacement therapy (CRRT) and intermittent hemodialysis (IHD) offer diverse benefits and drawbacks for critically ill children with acute kidney injury (AKI). Sustained low-efficiency daily diafiltration (SLEDD-f) involves a conceptual and technical hybrid of CRRT and IHD. We report our SLEDD-f application to critically ill children in the pediatric intensive care unit (PICU).
Methods: SLEDD-f was delivered by the new Fresenius 5008 therapy system with blood flow 5 ml/kg/min, dialysate flow 260 ml/min, hemofiltration 35 ml/kg/h for 8-10 h daily. Changes in blood pressure, blood gas, electrolyte, hemoglobulin (Hb), and hematocrit (Hct) were closely monitored.
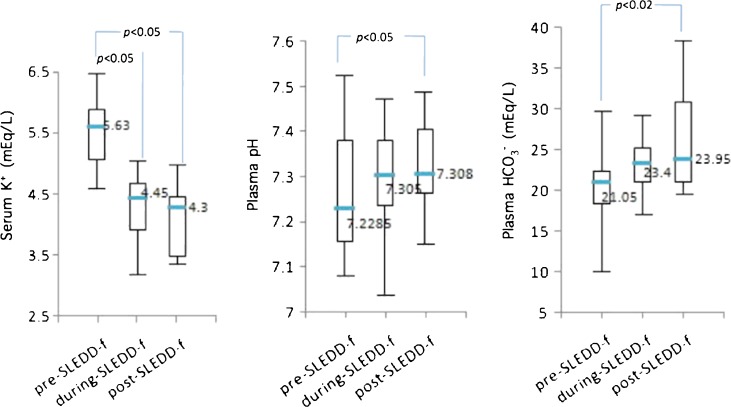
Results: From February 2010 to June 2011, 14 critical patients with a total of 60 SLEDD-f sessions were studied retrospectively. Heparin was used in 46 sessions (76.6%) with no bleeding complications. Hypertension above 135 mmHg returned to normal, hypotension below 90 mmHg showed no drop. Metabolic acidosis and hyperkalemia normalized. Elevated Hb, Hct, and their ratio revealed improving hemodilution. Three episodes of intradialytic hypotension (5.0%) and one of circuit clotting (1.7%) led to premature termination. The 28-day survival rate was 71.4%.
Conclusions: This pilot investigation demonstrates that SLEDD-f provides good hemodynamic tolerance and correction of fluid overload, pH, and electrolyte imbalance for critically ill children with AKI.
Figures




References
-
- Vanholder R, Van Biesen W, Lameire N. What is the renal replacement method of first choice for intensive care patients? J Am Soc Nephrol. 2001;12:S40–S43. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
