

Hepatitis B surface antigen concentrations in patients with HIV/HBV co-infection
- PMID: 22905219
- PMCID: PMC3419648
- DOI: 10.1371/journal.pone.0043143
Hepatitis B surface antigen concentrations in patients with HIV/HBV co-infection
Abstract
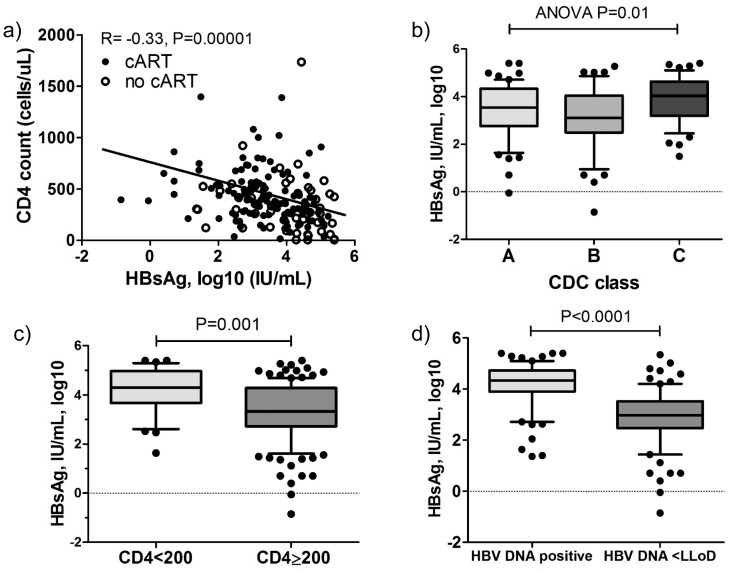
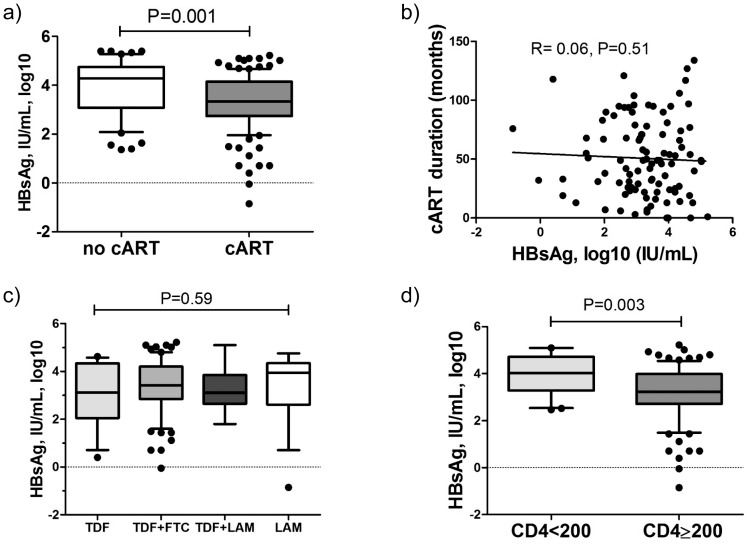
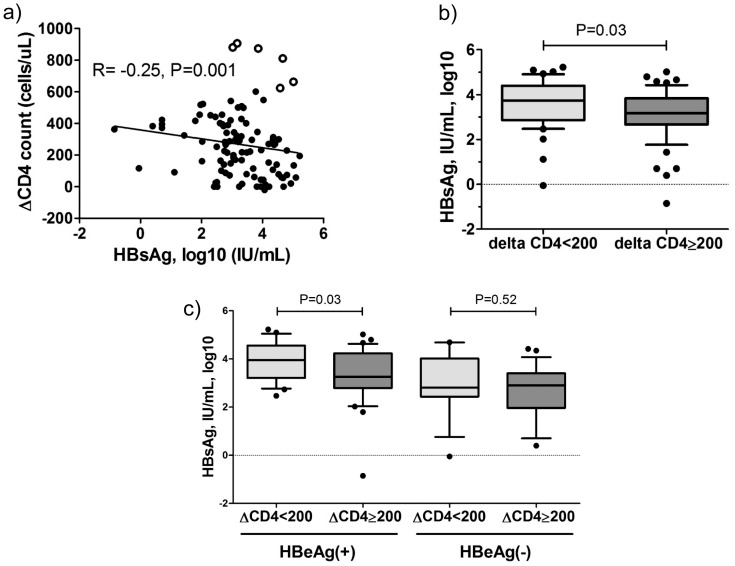
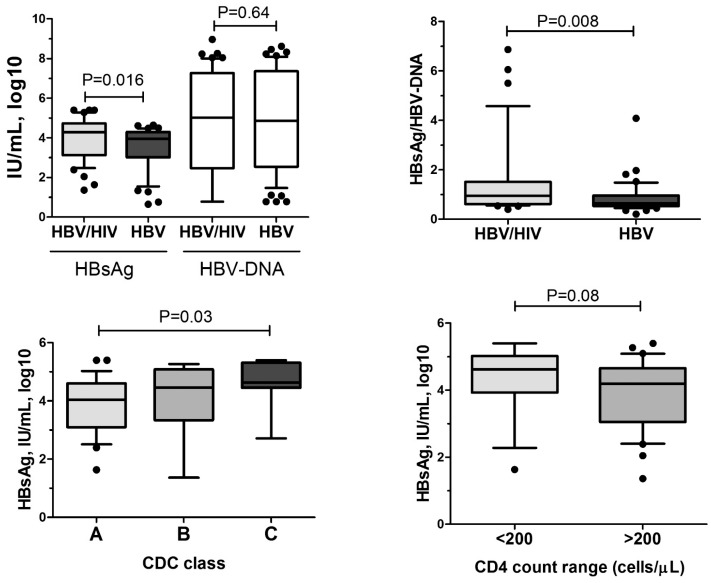
HBsAg clearance is associated with clinical cure of chronic hepatitis B virus (HBV) infection. Quantification of HBsAg may help to predict HBsAg clearance during the natural course of HBV infection and during antiviral therapy. Most studies investigating quantitative HBsAg were performed in HBV mono-infected patients. However, the immune status is considered to be important for HBsAg decline and subsequent HBsAg loss. HIV co-infection unfavorably influences the course of chronic hepatitis B. In this cross-sectional study we investigated quantitative HBsAg in 173 HBV/HIV co-infected patients from 6 centers and evaluated the importance of immunodeficiency and antiretroviral therapy. We also compared 46 untreated HIV/HBV infected patients with 46 well-matched HBV mono-infected patients. HBsAg levels correlated with CD4 T-cell count and were higher in patients with more advanced HIV CDC stage. Patients on combination antiretroviral therapy (cART) including nucleos(t)ide analogues active against HBV demonstrated significant lower HBsAg levels compared to untreated patients. Importantly, HBsAg levels were significantly lower in patients who had a stronger increase between nadir CD4 and current CD4 T-cell count during cART. Untreated HIV/HBV patients demonstrated higher HBsAg levels than HBV mono-infected patients despite similar HBV DNA levels. In conclusion, HBsAg decline is dependent on an effective immune status. Restoration of CD4 T-cells during treatment with cART including nucleos(t)ide analogues seems to be important for HBsAg decrease and subsequent HBsAg loss.
Conflict of interest statement
Figures
Similar articles
-
CD4+ T cell counts and soluble programmed death-1 at baseline correlated with hepatitis B surface antigen decline in HIV/HBV coinfection during combined antiretroviral therapy.Front Cell Infect Microbiol. 2023 May 3;13:1178788. doi: 10.3389/fcimb.2023.1178788. eCollection 2023. Front Cell Infect Microbiol. 2023. PMID: 37207191 Free PMC article.
-
Improved immune status corresponds with long-term decline of quantitative serum hepatitis B surface antigen in HBV/HIV co-infected patients.Viral Immunol. 2012 Dec;25(6):442-7. doi: 10.1089/vim.2012.0036. Epub 2012 Nov 6. Viral Immunol. 2012. PMID: 23131018
-
Differential T-cell profiles determined by Hepatitis B surface antigen decrease among people with Human Immunodeficiency Virus /Hepatitis B Virus coinfection on treatment.J Transl Med. 2024 Oct 4;22(1):901. doi: 10.1186/s12967-024-05681-y. J Transl Med. 2024. PMID: 39367456 Free PMC article.
-
Functional Cure of Hepatitis B Virus Infection in Individuals With HIV-Coinfection: A Literature Review.Viruses. 2021 Jul 11;13(7):1341. doi: 10.3390/v13071341. Viruses. 2021. PMID: 34372547 Free PMC article. Review.
-
Challenges and opportunities for hepatitis B cure in the setting of HIV--hepatitis B virus co-infection.Curr Opin HIV AIDS. 2020 May;15(3):193-199. doi: 10.1097/COH.0000000000000624. Curr Opin HIV AIDS. 2020. PMID: 32141889 Review.
Cited by
-
Chronic Hepatitis B and HIV Coinfection: A Continuing Challenge in the Era of Antiretroviral Therapy.Curr Hepatol Rep. 2020 Dec;19(4):345-353. doi: 10.1007/s11901-020-00541-x. Epub 2020 Sep 16. Curr Hepatol Rep. 2020. PMID: 33796434 Free PMC article.
-
HIV/HBV coinfection remodels the immune landscape and natural killer cell ADCC functional responses.Hepatology. 2024 Sep 1;80(3):649-663. doi: 10.1097/HEP.0000000000000877. Epub 2024 Apr 30. Hepatology. 2024. PMID: 38687604
-
The role of HBsAg levels in the current management of chronic HBV infection.Ann Gastroenterol. 2014;27(2):105-112. Ann Gastroenterol. 2014. PMID: 24733569 Free PMC article. Review.
-
HIV-HBV Coinfection-Current Challenges for Virologic Monitoring.Biomedicines. 2023 Apr 28;11(5):1306. doi: 10.3390/biomedicines11051306. Biomedicines. 2023. PMID: 37238976 Free PMC article. Review.
-
Occult hepatitis B virus infection in HIV positive patients at a tertiary healthcare unit in eastern India.PLoS One. 2017 Jun 7;12(6):e0179035. doi: 10.1371/journal.pone.0179035. eCollection 2017. PLoS One. 2017. PMID: 28591184 Free PMC article.
References
-
- European Association for the Study of the Liver (2012) EASL Clinical Practice Guidelines: management of chronic hepatitis B. J Hepatol. 57: 167–185. - PubMed
-
- Cornberg M, Jaroszewicz J, Manns MP, Wedemeyer H (2010) Treatment of chronic hepatitis B. Minerva Gastroenterol Dietol. 56: 451–465. - PubMed
-
- Chan HL, Thompson A, Martinot-Peignoux M, Piratvisuth T, Cornberg M, et al. (2011) Hepatitis B surface antigen Quantification: Why and How to use it in 2011 - A Core Group Report. J Hepatol 55: 1121–31. - PubMed
-
- Brunetto MR, Moriconi F, Bonino F, Lau GK, Farci P, et al. (2009) Hepatitis B virus surface antigen levels: a guide to sustained response to peginterferon alfa-2a in HBeAg-negative chronic hepatitis B. Hepatology. 49: 1141–1150. - PubMed
-
- Reijnders JG, Rijckborst V, Sonneveld MJ, Scherbeijn SM, Boucher CA, et al. (2010) Kinetics of hepatitis B surface antigen differ between treatment with peginterferon and entecavir. J Hepatol 54: 449–54. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
