

The lateral transpsoas approach to the lumbar and thoracic spine: A review
- PMID: 22905326
- PMCID: PMC3422088
- DOI: 10.4103/2152-7806.98583
The lateral transpsoas approach to the lumbar and thoracic spine: A review
Abstract
Background: In the last several years, the lateral transpsoas approach to the thoracic and lumbar spine, also known as extreme lateral interbody fusion (XLIF) or direct lateral interbody fusion (DLIF), has become an increasingly common method to achieve fusion. Several recent large series describe several advantages to this approach, including less tissue dissection, smaller incisions, decreased operative time, blood loss, shorter hospital stay, reduced postoperative pain, enhanced fusion rates, and the ability to place instrumentation through the same incision. Indications for this approach have expanded and now include degenerative disease, tumor, deformity, and infection.
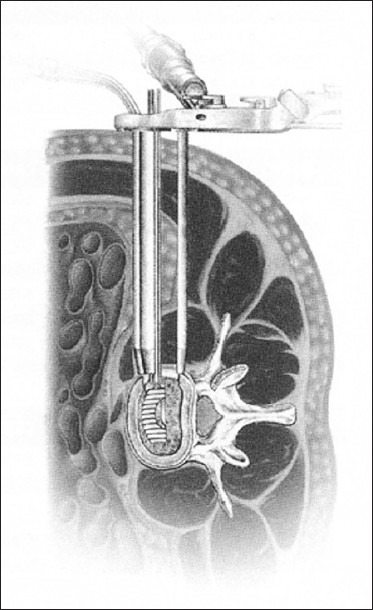
Methods: A lateral X-ray confirms that the patient is in a truly lateral position. Next, a series of tubes and dilators are used, along with fluoroscopy, to identify the mid-position of the disk to be incised. After continued dilation, the optimal site to enter the disk space is the midpoint of the disk, or a position slightly anterior to the midpoint of the disk. XLIF typically allows for a larger implant to be inserted compared to TLIF or PLIF, and, if necessary, instrumentation can be inserted percutaneously, which would allow for an overall minimally invasive procedure.
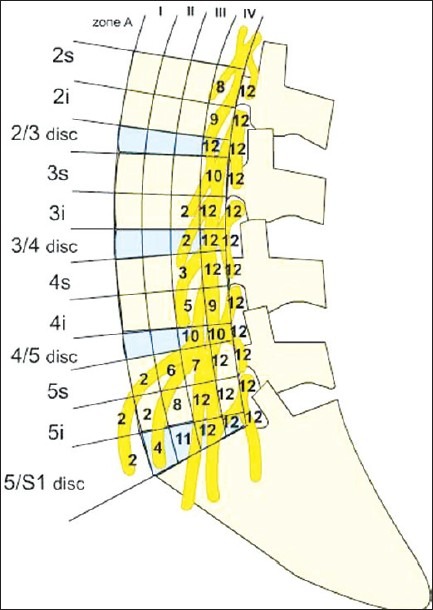
Results: Fixation techniques appear to be equal between XLIF and more traditional approaches. Some caution should be exercised because common fusion levels of the lumbar spine, including L4-5 and L4-S1, are often inaccessible. In addition, XLIF has a unique set of complications, including neural injuries, psoas weakness, and thigh numbness.
Conclusion: Additional studies are required to further evaluate and monitor the short and long-term safety, efficacy, outcomes, and complications of XLIF procedures.
Keywords: Lateral transpsoas approach; direct lateral interbody fusion; extreme lateral interbody fusion; lumbar spine; lumbosacral plexus; surgical technique.
Figures
References
-
- Acosta FL, Liu J, Slimack N, Moller D, Fessler R, Koski T. Changes in coronal and sagittal plane alignment following minimally invasive direct lateral interbody fusion for the treatment of degenerative lumbar disease in adults: A radiographic study. J Neurosurg Spine. 2011;15:92–6. - PubMed
-
- Anand N, Baron EM, Thaiyananthan G, Khalsa K, Goldstein TB. Minimally invasive multilevel percutaneous correction and fusion for adult lumbar degenerative scoliosis: A technique and feasibility study. J Spinal Disord Tech. 2008;21:459–67. - PubMed
-
- Anand N, Rosemann R, Khalsa B, Baron EM. Mid-term to long-term clinical and functional outcomes of minimally invasive correction and fusion for adults with scoliosis. Neurosurg Focus. 2010;28:E6. - PubMed
-
- Bagan B, Patel N, Deutsch H, Harrop J, Sharan A, Vaccaro AR, et al. Perioperative complications of minimally invasive surgery (MIS): Comparison of MIS and open interbody fusion techniques. Surg Technol Int. 2008;17:281–6. - PubMed
-
- Benglis DM, Vanni S, Levi AD. An anatomical study of the lumbosacral plexus as related to the minimally invasive transpsoas approach to the lumbar spine. J Neurosurg Spine. 2009;10:139–44. - PubMed
LinkOut - more resources
Full Text Sources
