

Splenic torsion requiring splenectomy six years following laparoscopic Nissen fundoplication
- PMID: 22906354
- PMCID: PMC3407447
- DOI: 10.4293/108680812X13291597716861
Splenic torsion requiring splenectomy six years following laparoscopic Nissen fundoplication
Abstract
Background: Laparoscopic Nissen fundoplication has become a mainstay in the surgical treatment of gastroesophageal reflux disease, as it has proved to be a durable, well-tolerated procedure. Despite the safety and efficacy associated with this procedure, surgeons performing this advanced laparoscopic surgery should be well versed in the potential intraoperative and postoperative complications.
Methods: A case is presented of a rare complication of splenic torsion following laparoscopic Nissen fundoplication. Diagnostic evaluations and intraoperative findings are discussed.
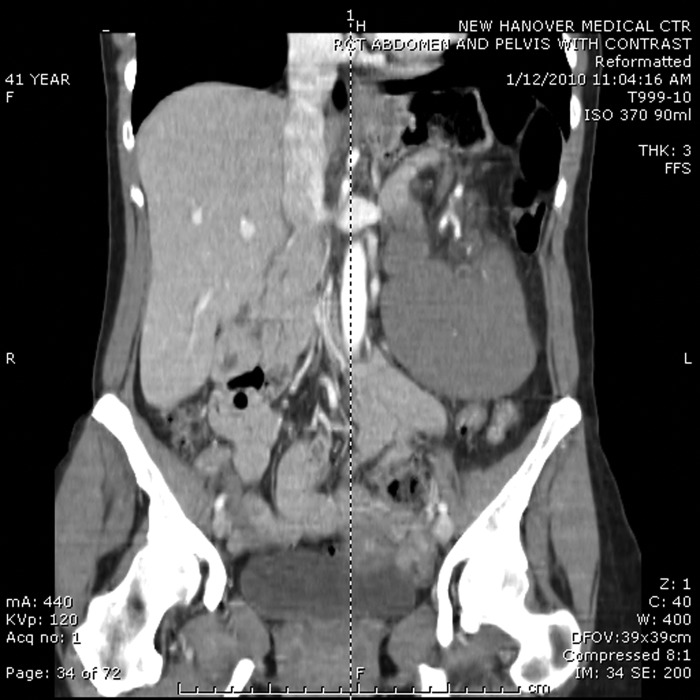
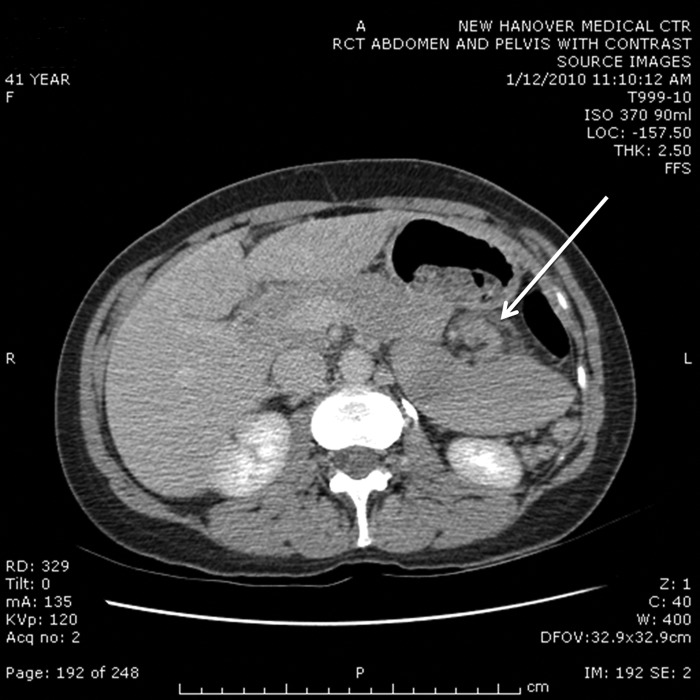
Results: We present an otherwise healthy 41-year-old woman who underwent a laparoscopic Nissen fundoplication 6 years earlier at another medical center and presented with worsening chronic left upper quadrant abdominal pain. She was diagnosed with torsion of the splenic vascular pedicle, resulting in heterogenicity of perfusion with associated hematoma requiring open splenectomy.
Conclusion: Surgeons should be aware of splenic torsion as a potential, albeit rare, complication related to laparoscopic Nissen fundoplication.
Figures


Similar articles
-
Postpartum splenic torsion in a patient with a wandering spleen and splenomegaly.BMJ Case Rep. 2025 Mar 3;18(3):e259196. doi: 10.1136/bcr-2023-259196. BMJ Case Rep. 2025. PMID: 40032560
-
Wandering spleen with splenic torsion in a toddler: A case report and literature review.Medicine (Baltimore). 2020 Sep 11;99(37):e22063. doi: 10.1097/MD.0000000000022063. Medicine (Baltimore). 2020. PMID: 32925740 Free PMC article. Review.
-
Splenic and parasplenic abscess as a late complication of laparoscopic nissen fundoplication--case report and review of the literature.Ann Acad Med Stetin. 2007;53(2):39-41. Ann Acad Med Stetin. 2007. PMID: 18557374 Review.
-
Two cases of pediatric splenic torsion as a possible late complication of laparoscopic fundoplication.Pediatr Int. 2024 Jan-Dec;66(1):e15810. doi: 10.1111/ped.15810. Pediatr Int. 2024. PMID: 39161211 No abstract available.
-
Wandering spleen with chronic torsion.Am J Surg. 2008 Apr;195(4):504-5. doi: 10.1016/j.amjsurg.2006.08.083. Am J Surg. 2008. PMID: 18070724
Cited by
-
Acute torsion of wandering spleen in a 17-year-old girl.Int J Clin Exp Med. 2015 Jul 15;8(7):11621-3. eCollection 2015. Int J Clin Exp Med. 2015. PMID: 26379994 Free PMC article.
-
'Wandering spleen with acute torsion' : a rare indication for splenectomy in an adult, complicated by postoperative splanchnic venous thrombosis and intestinal gangrene.BMJ Case Rep. 2021 Feb 4;14(2):e238647. doi: 10.1136/bcr-2020-238647. BMJ Case Rep. 2021. PMID: 33541983 Free PMC article.
-
Unusual gastric distention in a 1-year-old infant.J Am Coll Emerg Physicians Open. 2024 Feb 9;5(1):e13124. doi: 10.1002/emp2.13124. eCollection 2024 Feb. J Am Coll Emerg Physicians Open. 2024. PMID: 38343527 Free PMC article. No abstract available.
-
Acute abdomen due to torsion of the wandering spleen in a patient with Marfan Syndrome.World J Emerg Surg. 2013 Aug 5;8(1):30. doi: 10.1186/1749-7922-8-30. World J Emerg Surg. 2013. PMID: 23915457 Free PMC article.
-
Laparoscopic transperitoneal left adrenalectomy and wandering spleen risk.JSLS. 2014 Jul-Sep;18(3):e2014.00278. doi: 10.4293/JSLS.2014.00278. JSLS. 2014. PMID: 25392630 Free PMC article.
References
-
- Sodhi KS, Saggar K, Sood BP, Sandhu P. Torsion of a wandering spleen: acute abdominal presentation. J Emerg Med. 2003;25:133–137 - PubMed
-
- Misawa T, Yoshida K, Shiba H, Kobayashi S, Yanaga K. Wandering spleen with chronic torsion. Am J Surg. 2008;195:504–505 - PubMed
-
- Satyadas T, Nasir N, Bradpiece HA. Wandering spleen: case report and literature review. J R Coll Surg Edinb. 2002;47:512–514 - PubMed
-
- Vazquez JL, Montero M, Diaz F, Muguerza R, Paramo C, Rodriguez-Costa A. Acute torsion of the spleen: diagnosis and management. Pediatr Surg Int. 2004;20:153–154 - PubMed
-
- Dawson JH, Roberts NG. Management of the wandering spleen. Aust N Z J Surg. 1994;64:441–444 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical