

King's College Hospital Criteria for non-acetaminophen induced acute liver failure in an international cohort of children
- PMID: 22906509
- PMCID: PMC3504621
- DOI: 10.1016/j.jpeds.2012.07.002
King's College Hospital Criteria for non-acetaminophen induced acute liver failure in an international cohort of children
Abstract
Objective: To validate King's College Hospital criteria (KCHC) in children with non-acetaminophen induced pediatric acute liver failure (PALF) and to determine whether re-optimizing the KCHC would improve predictive accuracy.
Study design: We used the PALF study group database. Primary outcomes were survival without liver transplantation vs death at 21 days following enrollment. Classification and regression tree analysis was used to determine if modification of KCHC parameters would improve classification of death vs survival.
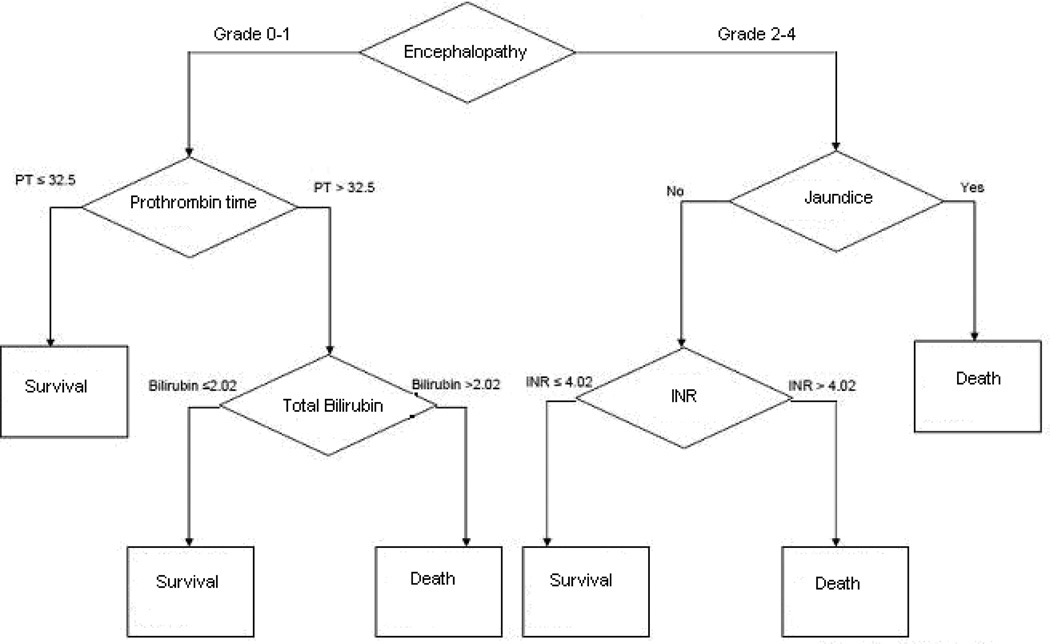
Results: Among 163 patients who met KCHC, 54 patients (33.1%) died within 21 days. Sensitivity of KCHC in this cohort was significantly lower than in the original study (61% vs 91%, P = .002), and specificity did not differ significantly. The positive predictive value (PPV) and negative predictive value (NPV) of KCHC for this cohort was 33% and 88% respectively. Classification and regression tree analysis yielded the following optimized parameters to predict death: grade 2-4 encephalopathy, international normalized ratio >4.02, and total bilirubin >2.02 mg/dL. These parameters did not improve PPV, but NPV was significantly better (88% vs 92%, P < .0001).
Conclusions: KCHC does not reliably predict death in PALF. With a PPV of 33%, twice as many participants who met KCHC recovered spontaneously than died, indicating that using KCHC may cause over utilization of liver transplantation. Re-optimized cutpoints for KCHC parameters improved NPV, but not PPV. Parameters beyond the KCHC should be evaluated to create a predictive model for PALF.
Copyright © 2013 Mosby, Inc. All rights reserved.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Durand P, Debray D, Mandel R, Baujard C, Branchereau S, Gauthier F, et al. Acute liver failure in infancy: a 14-year experience of a pediatric liver transplantation center. J Pediatr. 2001;139:871–876. - PubMed
-
- Russell GJ, Fitzgerald JF, Clark JH. Fulminant hepatic failure. J Pediatr. 1987;111:313–319. - PubMed
-
- Ostapowicz G, Fontana RJ, Schiodt FV, Larson A, Davern TJ, Han SH, et al. Results of a prospective study of acute liver failure at 17 tertiary care centers in the United States. Ann Intern Med. 2002;137:947–954. - PubMed
-
- Devictor D, Desplanques L, Debray D, Ozier Y, Dubousset AM, Valayer J, et al. Emergency liver transplantation for fulminant liver failure in infants and children. Hepatology. 1992;16:1156–1162. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- UL1 TR000005/TR/NCATS NIH HHS/United States
- UL1 RR024153/RR/NCRR NIH HHS/United States
- MO1 RR08084/RR/NCRR NIH HHS/United States
- M01 RR000069/RR/NCRR NIH HHS/United States
- MO1 RR00069/RR/NCRR NIH HHS/United States
- UL1 RR02501-04/RR/NCRR NIH HHS/United States
- UL1RR024153/RR/NCRR NIH HHS/United States
- U01-DK072146-05/DK/NIDDK NIH HHS/United States
- UL1 TR000077/TR/NCATS NIH HHS/United States
- U01 DK072146/DK/NIDDK NIH HHS/United States
- UL1 RR024131/RR/NCRR NIH HHS/United States
- M01 RR008084/RR/NCRR NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
